


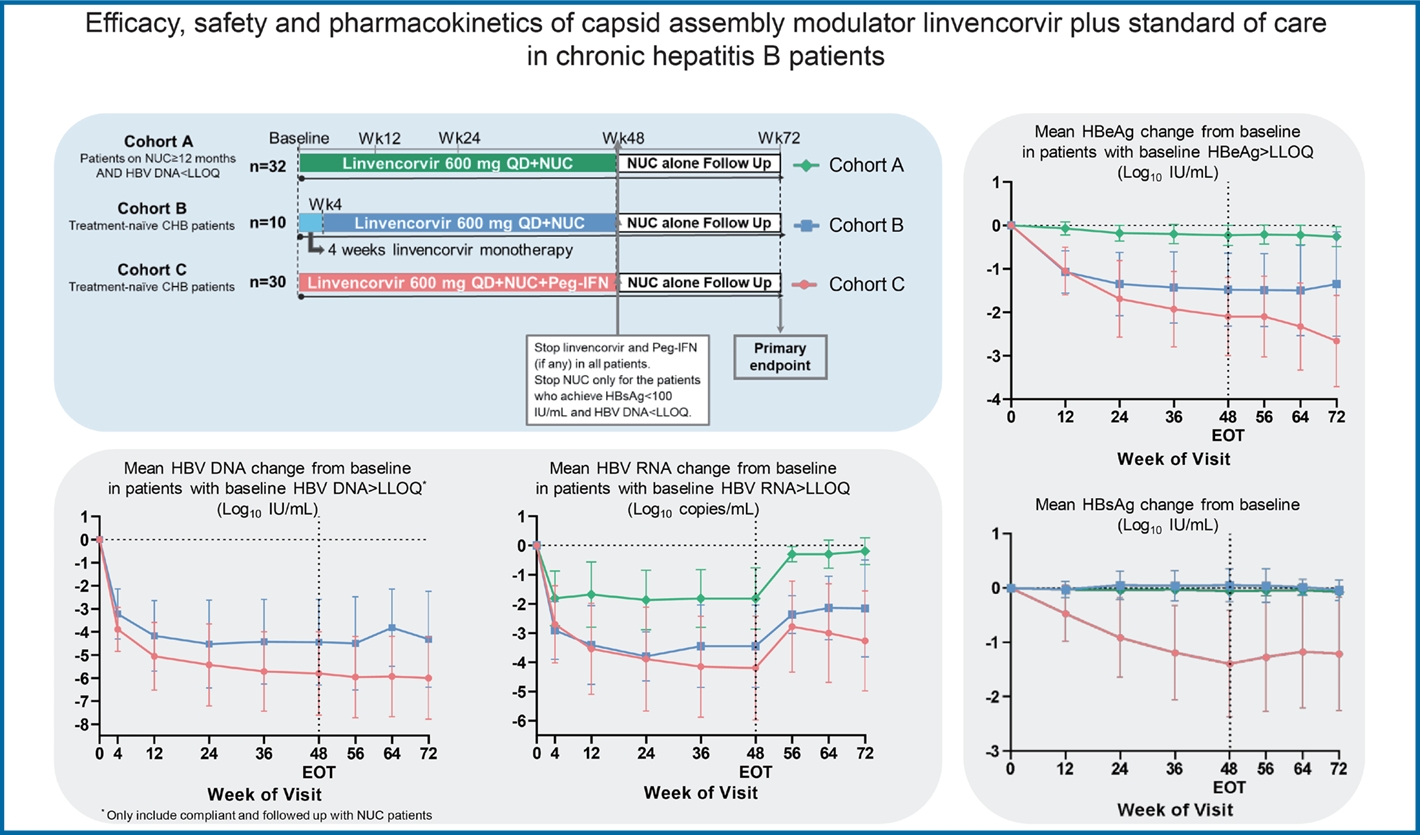
Graphical Abstract
INTRODUCTION
Hepatitis B virus (HBV) infection remains a major global health challenge, and is associated with life-threatening consequences [1,2]. Functional cure, defined as unquantifiable HBV DNA and sustained hepatitis B surface antigen (HBsAg) loss [3], improves long-term prognosis and is a major therapeutic goal for chronic hepatitis B (CHB) therapy [4-7]. Currently available treatments for CHB, including nucleos(t)ide analogues (NUCs) and pegylated interferon (Peg-IFN), have limitations. NUCs, which inhibit HBV DNA synthesis, are unable to fully suppress viral replication in some patients (or do so very slowly), especially in hepatitis B e antigen (HBeAg) positive patients and those with high viral load [8,9]. NUCs must be taken life-long, have no direct effect on HBV RNA or covalently closed circular DNA (cccDNA), and rarely lead to functional cure [3,5,7,10,11]. Peg-IFN therapy is finite, but results in low rates of functional cure and is associated with side effects [12]. There is therefore a need for novel, well tolerated treatments that can augment viral suppression and help clear HBsAg in combination with current standard of care (SoC) [10].
The HBV capsid is involved in multiple steps of the HBV life cycle and is an important target of antiviral therapies in development [13,14]. Several capsid assembly modulators (CAMs), which inhibit viral replication by inducing the formation of aberrant non-capsid polymers (CAM-A, previously known as Class I) or morphologically normal but nucleic acid-free empty capsids (CAM-E, previously known as Class II) [15], have reached phase 1 and 2 clinical development [13]. Studies to date have shown that 24-week treatment with CAM and NUC leads to suppression of HBV DNA and RNA, but has limited effect on HBV antigens [14,16,17].
Linvencorvir (RO7049389) is a novel small molecule CAM that induces aberrant capsid assembly, leading to the degradation of viral core protein, thereby inhibiting pregenomic RNA (pgRNA) encapsidation and HBV DNA replication. Further, linvencorvir also induces the disassembly of nucleocapsids, potentially interfering with cccDNA biosynthesis [18]. A first-in-human, three-part phase 1/2 study of linvencorvir has been conducted in healthy volunteers and CHB patients. In Part 1 of the phase 1/2 study, linvencorvir showed favourable safety and pharmacokinetic profiles in healthy volunteers following single ascending doses up to 2,500 mg, and multiple ascending doses up to 1,200 mg/day for 2 weeks [19]. In Part 2, 4-week monotherapy with linvencorvir up to 1,000 mg/day was generally safe and well tolerated, and had potent antiviral activity in viremic CHB patients [20]. Here, we report Part 3 (phase 2 stage) of the phase 1/2 study, in which we evaluated the efficacy, safety and pharmacokinetics of linvencorvir in combination with SoC therapies (NUC with or without Peg-IFN-α) for 48 weeks in virologically-suppressed and treatment-naïve CHB patients.
MATERIALS AND METHODS
Study design and population
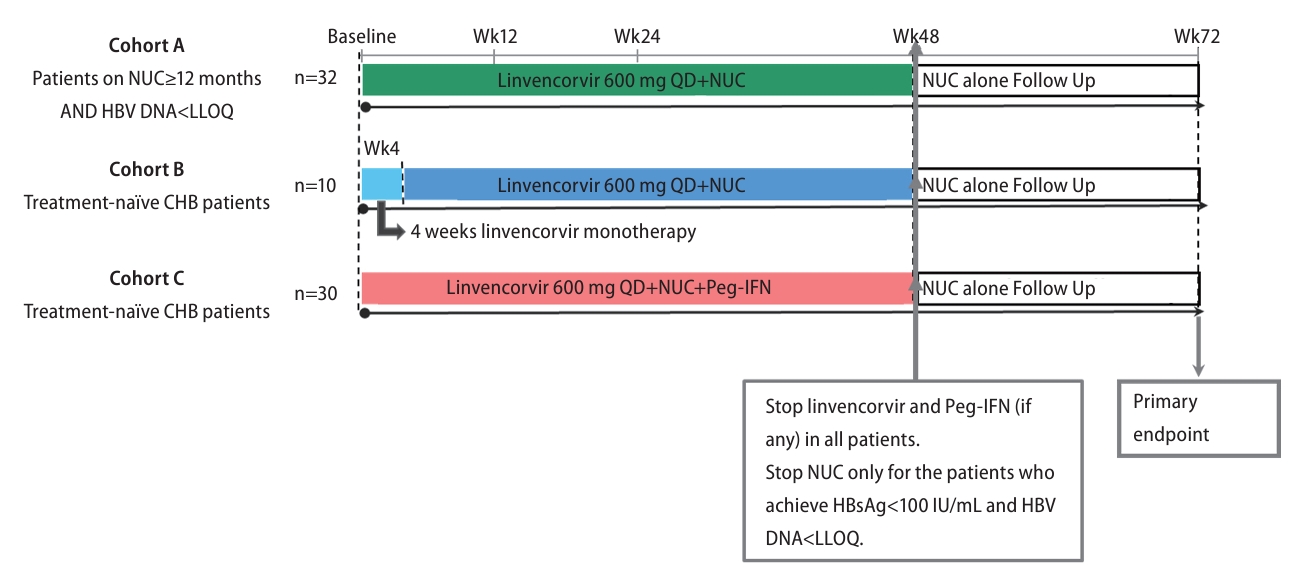
This multicenter, non-randomized, non-controlled, open-label phase 2 study (Part 3 of the first-in-human linvencorvir trial) was performed at 16 sites in Taiwan (n=5), Mainland China (n=3), New Zealand (n=2), Thailand (n=2), Australia (n=1), Bulgaria (n=1), Hong Kong (n=1) and Singapore (n=1). This study comprised three treatment cohorts, in which NUC-suppressed or treatment-naïve CHB patients received open-label treatment with linvencorvir plus a first-line NUC (entecavir [ET V], tenofovir alafenamide [TAF], or tenofovir disoproxil fumarate [TDF]) with or without Peg-IFN-α for 48 weeks (Fig. 1). In Cohort A, NUC-suppressed patients received linvencorvir plus NUC therapy for 48 weeks. In Cohort B, treatment-naïve patients received linvencorvir alone for the first 4 weeks of the treatment period, followed by linvencorvir plus NUC therapy for the remaining 44 weeks. Treatment-naïve patients enrolled in Cohort C received linvencorvir plus NUC and Peg-IFN-α therapy throughout the 48-week study treatment period. After the study treatment period, all patients were followed up for 24 weeks with NUC monotherapy, or without NUC if they met protocol-defined NUC stopping criteria (HBsAg below 100 IU/mL and HBV DNA below the lower limit of quantification [LLOQ; 20 IU/mL]) at the end of study treatment (Week 48). During the off-treatment follow-up period, if alanine aminotransferase (ALT) >2 times the upper limit of normal (ULN; 41 U/L for men and 33 U/L for women) was accompanied by confirmed virological relapse, NUC treatment may be restarted at the discretion of the investigator and applicable CHB guidelines.
Eligible patients were aged 18ŌĆō60 years with CHB (a positive HBsAg or HBV DNA test or HBeAg-positive for more than 6 months before screening), and HBsAg concentration above 250 IU/mL at screening. NUC-suppressed patients were required to have been treated with NUC monotherapy (ETV, TAF, or TDF) for at least 12 months, and must have been on the same NUC therapy for at least 3 months before screening. These patients should have HBV DNA below LLOQ at screening, and ALT Ōēż2├ŚULN at screening and Day -1. Treatment-na├»ve patients were required to have previously received anti-HBV treatments for less than 30 days in total, and to have not received any anti-HBV treatment within 3 months prior to the first study dose. Treatment-na├»ve patients also required HBV DNA of at least 2├Ś104 IU/mL (HBeAg-positive patients) or 2├Ś103 IU/mL (HBeAg-negative patients) at screening, and ALT levels between 1ŌĆō5├ŚULN at screening and below 5├ŚULN at Day -1. Full details of the eligibility criteria are provided in the Supplementary Material.
The study was conducted in accordance with Good Clinical Practice standards and the Declaration of Helsinki. The study protocol was approved by the institutional review boards or ethics committees from all participating study centres, and written informed consent was obtained from each participant included in the study.
Procedures
In all three treatment cohorts, linvencorvir 600 mg was administered orally once a day in the fasted state (Ōēź2 hours after a meal and Ōēź2 hours before the next meal). NUC (ETV, TAF, or TDF) and Peg-IFN-╬▒ therapy were administered according to the local label or guidelines. Investigators could refer to Peg-IFN stopping rules recommended in major guidelines [5,7,21]. If Peg-IFN was stopped before the end of the 48-week treatment period, linvencorvir and NUC were to be continued until the end of the treatment period. At the end of the study treatment period, NUC therapy was continued for 24 weeks unless patients met the NUC stopping criteria.
Safety-related clinical and laboratory evaluations, and blood sample collections for the determination of HBV viral dynamic responses were conducted on day-1, during the study treatment period (every 2 weeks for the first 4 weeks and every 4 weeks thereafter), and during the follow-up (every 8 weeks for patients not meeting the NUC stopping criteria; every 2 weeks for the first 12 weeks and every 4 weeks thereafter for patients meeting the NUC stopping criteria). Details of methodologies for determining HBV genotype, and measuring viral dynamic markers are provided in the Supplementary Material. In particular, plasma HBV RNA was quantitatively assessed at Roche Diagnostic International Ltd (for non-Chinese sites) or Q2 Solutions for Chinese sites using a COBAS® HBV RNA test on the Roche COBAS® 6800 System [22,23]. Safety assessments included monitoring and recording the occurrence and severity of adverse events (AEs), physical examinations, safety laboratory assessments, vital signs, and 12-lead electrocardiograms (ECGs). AEs and ALT and aspartate aminotransferase (AST) elevations were graded according to the Division of AIDS criteria (Supplementary Table 1).
Plasma samples for pharmacokinetics (PK) analysis were collected at the following time points: (1) pre-dose and 1ŌĆō8 hours post-dose on day 1 and Weeks 4 (Cohort B only) and 24, (2) pre-dose and 1ŌĆō4 hours post-dose at all other scheduled visits during study treatment; and (3) before and 1ŌĆō24 hours after the last dose of study treatment.
Endpoints
The primary endpoint in this study was HBV DNA below the LLOQ (20 IU/mL) with HBsAg loss (<0.05 IU/mL) at 24 weeks post-treatment (defined as functional cure in the protocol). Secondary efficacy endpoints included serum HBV DNA and RNA below the LLOQ, HBsAg and HBeAg loss and anti-HBs and anti-HBe seroconversion, quantitative change from baseline for the HBV markers including serum HBV DNA, HBV RNA and HBV antigens. Secondary efficacy endpoints were assessed in each cohort overall and the following patient subgroups: HBeAg-positive and HBeAg-negative, and low and high baseline HBsAg (cutoff: 4 log10 IU/mL). Relationships between secondary efficacy endpoints and HBV genotype and high baseline HBV DNA (>7 log10 IU/mL) were also explored. Other secondary endpoints were the incidence of AEs and most common AEs, and the PK profile of linvencorvir and its metabolites when used in combination with SoC therapies.
Statistical analysis
The sample size for this study was intended to support the assessment of the functional cure rate. Individual cohort sample sizes of at least 10ŌĆō30 were planned to ensure that the lower 95% confidence interval was above 5ŌĆō14% if there was an observed functional cure rate of 30%, assuming binomial distribution.
All patients who received at least one dose of linvencorvir were included in the safety and efficacy analysis populations. Efficacy analyses were based on the actual number of patients with valid results at each study visit. For the PK analysis, patients who significantly violated inclusion or exclusion criteria, who deviated significantly from the protocol, or for whom data were unavailable or incomplete which may have influenced the PK analysis were excluded.
For continuous variables, descriptive statistics were calculated. Values below the LLOQ were imputed to numeric values below the LLOQ value to make a conservative calculation of change from baseline values (Supplementary Table 2). For categorical data, the number and proportion of study participants in each category were summarized. SpearmanŌĆÖs rank correlation was calculated to determine the relationship between graded treatment-emergent ALT elevations and categorized maximal declines in HBsAg. PK parameters were calculated from a non-compartment analysis using Phoenix software (WinNonlin models version 6.4).
RESULTS
Patient characteristics
Between June 14, 2019 and October 19, 2020, 72 (44%) of 163 screened patients were enrolled in the study: 32 NUC-suppressed patients in Cohort A, 10 and 30 treatment-naïve patients in Cohorts B and C, respectively (Fig. 2). All 72 patients received linvencorvir, and 68 (94.4%) patients completed the 72-week study. Linvencorvir treatment was discontinued early for non-safety reasons in four patients (on days 15 and 62 for two patients in Cohort A, and on days 83 and 237 for two patients in Cohort C).
Baseline demographics and clinical characteristics are shown in Table 1. In Cohorts A and C, patients were predominantly Asian and male, whereas 5 (50%) patients were Asian and 5 (50%) patients were male in Cohort B. HBV DNA levels were below the LLOQ in all Cohort A patients, but 15 (46.9%) patients had quantifiable HBV RNA. Mean baseline HBV DNA levels were 5.73 log10 IU/mL in Cohort B and 6.91 log10 IU/mL in Cohort C. Two (20%) and 18 (60%) patients in Cohorts B and C, respectively, had a high viral load (HBV DNA >7 log10 IU/mL). Eight (80%) and 27 (90%) patients in Cohorts B and C, respectively, had baseline quantifiable HBV RNA. In Cohort A, six (19%) patients had HBV genotype C, as did five patients (50%) in Cohort B, and 11 patients (37%) in Cohort C. NUC-suppressed patients were mainly HBeAg-negative (66% [21/32]), but treatment-na├»ve patients were mainly HBeAg-positive (63% [25/40]). Mean baseline HBsAg levels across the three cohorts ranged from 3.2 log 10 IU/mL in Cohort A to 3.96 log10 IU/mL in Cohort C. More than half of the Cohort C patients had high baseline HBsAg levels (Ōēź 4 log10 IU/mL).
Primary endpoint
In this study, no patient achieved HBV DNA<LLOQ with HBsAg loss at Week 24 post-study treatment (functional cure).
HBV DNA responses
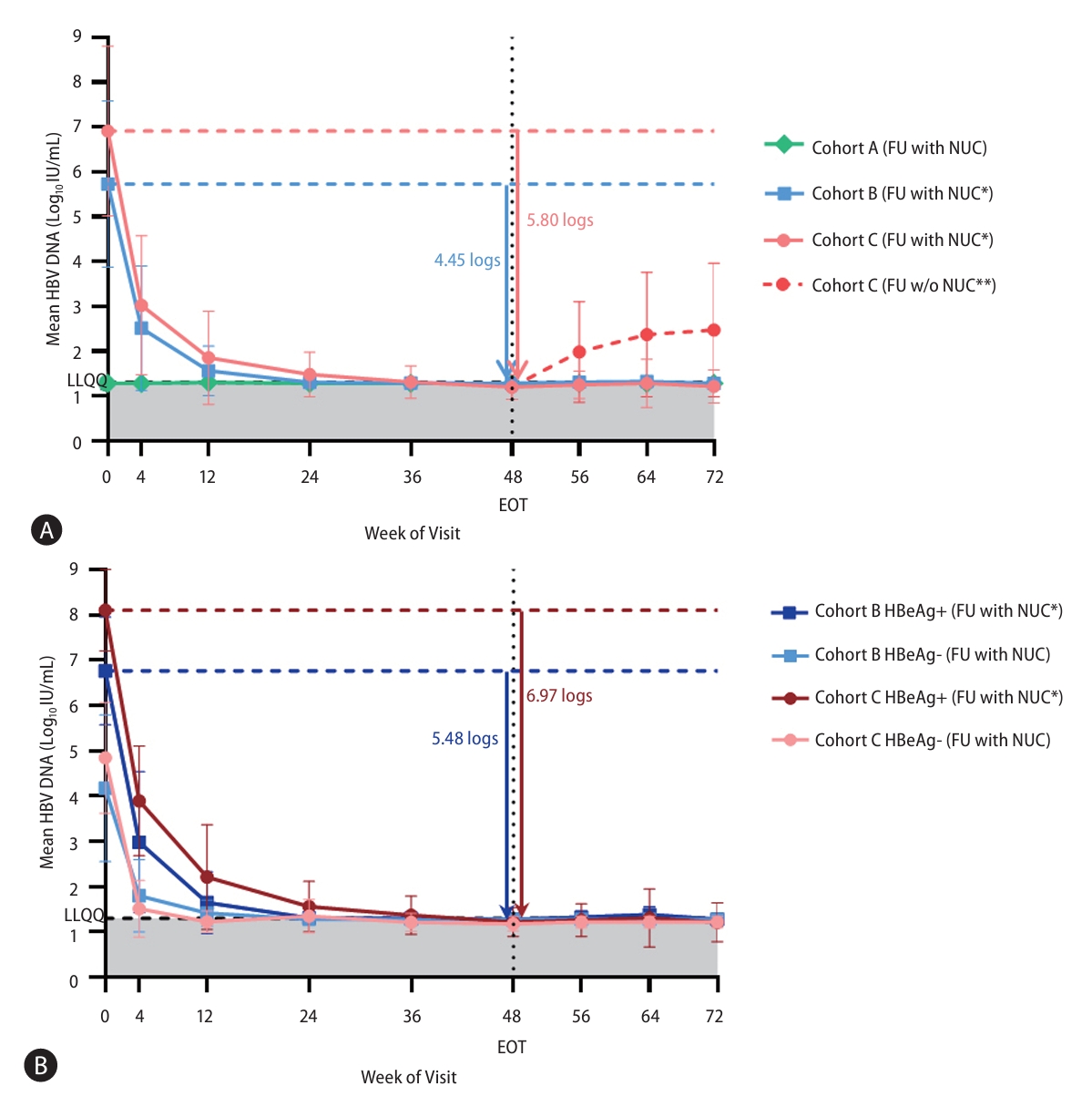
In NUC-suppressed patients (Cohort A), mean HBV DNA levels remained below the LLOQ throughout the study. In treatment-na├»ve patients, HBV DNA levels declined by a mean (standard deviation [SD]) of 4.45 (1.86) and 5.80 (1.81) log10 IU/mL at Week 48 in Cohorts B and C, respectively (Fig. 3A). With higher baseline HBV DNA levels, HBeAg-positive patients achieved larger reductions in HBV DNA than HBeAg-negative patients (mean [SD] HBV DNA declines of 5.48 [1.19] vs. 2.90 [1.62] log10 IU/mL, respectively, in Cohort B; 6.97 [0.74] vs. 3.80 [1.20] log10 IU/mL, respectively, in Cohort C) (Fig. 3B). All ten (100%) Cohort B patients achieved HBV DNA below the LLOQ at Week 48, including two HBeAg-positive patients with high viral load. By Week 48, HBV DNA levels reached below the LLOQ in 86% (24/28) of Cohort C patients who completed 48-weeks of study treatment, including in 76% (13/17) of HBeAg-positive patients with high viral load. All the remaining four patients who had not achieved unquantifiable HBV DNA during the study treatment had significantly reduced viral DNA levels (<150 IU/mL) at Week 48. At the end of study treatment, all Cohort B patients entered into the 24-week follow-up with NUC treatment. Five patients in Cohort C met the NUC stopping criteria at Week 48, so they were followed without NUC. During the NUC-alone follow-up period, 96% (26/27) of NUC-compliant Cohorts B and C patients with unquantifiable HBV DNA by Week 48 sustained HBV DNA below the LLOQ; the four patients who had not achieved unquantifiable HBV DNA by Week 48 attained HBV DNA below the LLOQ or maintained low HBV DNA levels. Among the five patients who entered off-treatment follow-up, four patients experienced HBV DNA rebound to quantifiable levels at around Week 56. Three out of them were not retreated at the investigatorsŌĆÖ discretion and the remaining patient restarted NUC treatment from Week 60 with HBV DNA subsequently declining to below the LLOQ.
HBV RNA responses
Among the patients with quantifiable baseline HBV RNA, HBV RNA levels were suppressed to below the LLOQ at Week 48 in 93% (14/15), 100% (8/8) and 88% (22/25) of patients in Cohorts A, B and C, respectively. The mean (SD) 48-week declines in HBV RNA for patients with quantifiable baseline HBV RNA were 1.82 (1.05) log10 copies/mL in Cohort A, 3.45 (1.41) log10 copies/mL in Cohort B, and 4.20 (1.78) log10 copies/mL in Cohort C (Fig. 4). During the follow-up without linvencorvir, HBV RNA levels rebounded to approximately the baseline levels in Cohort A patients, but mean reductions from baseline of 2.16 (1.66) and 3.27 (1.71) log10 copies/mL were retained at Week 72 in Cohorts B and C patients, respectively. Patients in all three cohorts with unquantifiable baseline HBV RNA maintained HBV RNA levels below the LLOQ during the study treatment and NUC-alone follow-up periods.
HBsAg responses
No HBsAg loss or anti-HBs seroconversion occurred among patients completing the study. No apparent mean declines for Cohort A and B in HBsAg were observed during the study (Fig. 5A), but two HBeAg-positive patients in Cohort B had maximal HBsAg declines of 0.40ŌĆō0.45 log10 IU/mL. In Cohort C, at Week 48, mean (SD) HBsAg decline was 1.39 (0.98) log10 IU/mL and numerically larger mean (SD) HBsAg declines occurred in HBeAg-positive and patients with baseline HBsAg Ōēź4 log10 IU/mL (1.64 [0.90] log 10IU/mL and 1.72 [0.88] log10 IU/mL, respectively). HBV genotype B and C patients achieved mean (SD) HBsAg declines of 1.35 (0.62) and 1.74 (1.13) log10 IU/mL from baseline levels of 3.80 (0.76) and 4.41 (0.91) log10 IU/mL, respectively (Table 2, Fig. 5A). At Week 48, 21% (6/28) and 68% (19/28) of patients achieved HBsAg levels <2 and 3 log10 IU/mL, respectively (Table 2). HBsAg declines were concurrent with treatment-emergent grade 2ŌĆō4 ALT elevations which mostly occurred in treatment-na├»ve patients, with statistically significant positive correlations between graded ALT elevations and categorical maximal HBsAg declines (SpearmanŌĆÖs rho 0.432, P=0.017 for Cohort C and 0.697, P=0.025 for Cohort B) (Supplementary Fig. 1).
HBeAg and HBcrAg responses
At Week 48, NUC-suppressed HBeAg-positive Cohort A patients had mean (SD) HBeAg decline of 0.23 (0.23) log10 IU/mL from 0.41 (0.75) log10 IU/mL at baseline. Treatment-naïve, HBeAg-positive Cohorts B and C patients had mean (SD) HBeAg declines of 1.48 (0.84) and 2.10 (0.90) log10 IU/mL, respectively (Fig. 5B). Among the HBeAg-positive treatment-naïve patients, 50% (3/6) and 39% (7/18) achieved HBeAg loss and anti-HBe seroconversion occurred in 17% (1/6) and 33% (6/18) in Cohorts B and C, respectively. At Week 48, HBcrAg levels declined from baseline by mean (SD) of 0.13 (0.24), 1.23 (0.76), and 1.76 (1.1) log10 U/mL in Cohorts A, B, and C, respectively (Fig. 5C). During the follow-up period, levels of HBeAg and HBcrAg were generally sustained in treatment-naïve patients.
Adverse events
AEs occurred in 69% (22/32) of NUC-suppressed patients in Cohort A, 90% (9/10) of treatment-na├»ve patients in Cohort B, and all 30 treatment-na├»ve patients in Cohort C (Table 3). Headache, pyrexia, and increased ALT levels were among the most commonly reported AEs. Increased ALT levels occurred mainly at Weeks 2ŌĆō8, and resolved within 14 weeks with no accompanying bilirubin/indirect bilirubin increase, although a mild increase in bilirubin occurred in a NUC-suppressed patient who had pre-existing liver disease (cholestasis and Gilbert syndrome). Moreover, in all five patients with grade 4 ALT elevations, linvencorvir was interrupted per protocol, but no further ALT elevations occurred after re-administering. Most AEs were grades 1ŌĆō2. Grade 3ŌĆō4 AEs were reported in four Cohort A patients (13%), two Cohort B patients (20%), and 11 Cohort C patients (37%). There were eight serious AEs and one death (due to malignant melanoma), none of which were related to linvencorvir. Most treatment-related AEs occurred in Cohort C: 74 related to linvencorvir, 25 related to NUC and 266 related to Peg-IFN-╬▒. Four AEs were assessed as being related to linvencorvir in each of Cohorts A and B (Table 3). There were no trends of clinically significant changes in vital signs or ECG data.
Pharmacokinetics
Linvencorvir was rapidly absorbed and eliminated, with low accumulation of linvencorvir and its major metabolites in plasma after 48 weeks of dosing. The PK profiles of linvencorvir, with or without SoC (NUC with or without Peg-IFN-╬▒), were considered similar. The plasma concentration of NUCs and Peg-IFNs remained stable during the study treatment period.
DISCUSSION
In this study, no patient achieved functional cure at 24 weeks post-48-week treatment with linvencorvir 600 mg/day plus NUC with or without Peg-IFN-α. Linvencorvir plus NUC with or without Peg-IFN-α did demonstrate potent suppression of HBV DNA and RNA. Linvencorvir plus NUC and PEG-IFN-α in treatment-naïve patients led to the greatest overall declines in HBV antigens. Linvencorvir was generally safe and well tolerated in combination with SoC.
HBV DNA was maintained below the LLOQ throughout the study in NUC-suppressed patients and was suppressed below the LLOQ in the majority of treatment-na├»ve patients, including HBeAg-positive patients with high viral load. Moreover, after linvencorvir cessation, HBV DNA generally remained suppressed by NUC monotherapy. While complete suppression of HBV DNA is an essential part of functional cure, 30% to 50% HBeAg positive and/or patients with high viral load cannot achieve HBV DNA<LLOQ with 1ŌĆō3 years NUC monotherapy. Furthermore, some CHB patients may develop low-level viremia even with long-term NUC treatment [7-9]. For these NUC difficult-to-treat patients, addition of linvencorvir to NUC may be a potential therapeutic strategy. Larger and longer trials would be necessary to test this hypothesis.
Serum HBV RNA was suppressed to below the LLOQ in the majority of NUC-suppressed and treatment-naïve patients during study treatment, which reflected target engagement by linvencorvir. During the off-linvencorvir follow-up period, retained HBV RNA declines were only observed in treatment-naïve patients, suggesting that initial HBV RNA declines in treatment-naïve patients may be more readily retained than secondary declines in NUC-suppressed patients. This partially sustained HBV RNA suppression, together with durable declines in HBcrAg and HBeAg, may indicate suppression of cccDNA transcriptional activity or a reduction in cccDNA levels [24,25], which is rarely observed in NUC therapy alone [26]. Consistent with this hypothesis, CAMs have been shown in vitro to induce disassembly of nucleocapsids, thereby interfering with cccDNA reservoir establishment and replenishment [26-28].
Linvencorvir showed little benefit in HBsAg reduction on top of NUC, however, when combined with Peg-IFN-α, HBsAg declines were observed in treatment-naïve patients. Notably, the HBsAg mean decline observed in Cohort C was larger than it was in a previous study of TDF plus Peg-IFN combination therapy [29]. Moreover, HBsAg levels declined comparably in Cohort C patients with HBV genotypes C and B. It has been reported that HBsAg decline was significantly lower in patients with either HBV genotypes C or D than in patients with HBV genotypes A and B with one-year Peg-IFN plus NUC treatment [30,31]. However, due to the limited sample size, the baseline differences, and the lack of a control group of Peg-IFN plus NUC, any additional benefit to HBsAg reduction from linvencorvir on top of Peg-IFN and NUC needs to be confirmed.
There were no unexpected safety concerns when linvencorvir was administered in combination with NUC or NUC plus Peg-IFN-α. AEs occurring in patients receiving linvencorvir plus NUC and Peg-IFN-α were consistent with the safety profile of Peg-IFN-α. As the observations seen in the previous study with 4-week linvencorvir monotherapy [20], transient treatment-emergent ALT elevations were observed almost exclusively in treatment-naïve patients but not in NUC-suppressed patients, and were accompanied by declining levels of viral antigens, including HBsAg. These ALT elevations are consistent with the natural history of CHB patients with active viral replication and are considered indicators of the host immune response against HBV rather than drug-induced liver injury [32-34].
Limitations of this study include its non-randomized, non-controlled design with no stratification, as well as the small sample size. The small sample size and unbalanced baseline characteristics detract from the validity of subgroup analyses.
In conclusion, linvencorvir is generally safe and well tolerated when added to SoC therapy for CHB. Linvencorvir on top of SoC potently suppresses HBV replication, including in HBeAg-positive patients and those with high viral load, however limited benefit is shown towards HBsAg loss. Next-generation CAMs with higher potency and greater inhibitory activity towards cccDNA reservoir maintenance may result in different outcomes towards the achievement of functional cure in CHB patients.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement1
Supplement1 Print
Print





