


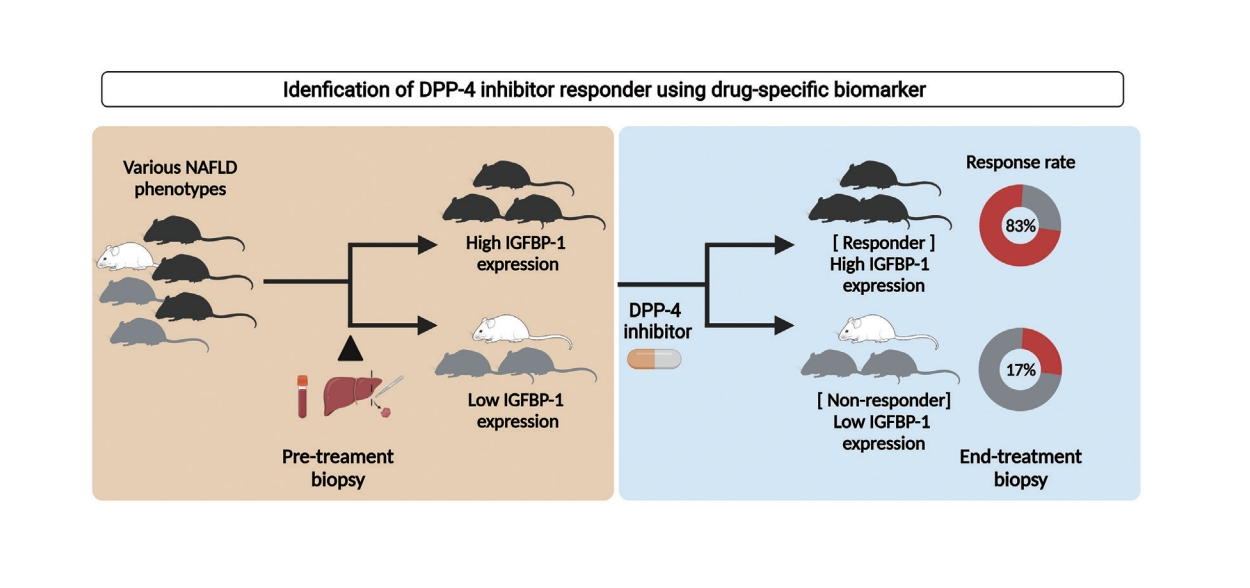
Graphical Abstract
INTRODUCTION
Non-alcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease. The overall prevalence of NAFLD in Asian countries is approximately 29.6% [1]. Approximately 30% of NAFLD cases are accompanied by steatohepatitis or fibrosis, leading to the progression of liver disease. Annual medical costs and the socioeconomic burden associated with NAFLD have increased sharply in the United States [2].
No drugs have been approved for the treatment of NAFLD. Several phase IIb and III clinical trials are ongoing; however, the results are unsatisfactory [3]. One of the main reasons for this is the heterogeneity of the patients with NAFLD. There are diverse phenotypes and complex pathophysiologies in patients with NAFLD. There are diverse phenotypes and complex pathophysiologies in patients with NAFLD, which must be targeted precisely to treat them effectively [4,5]. However, current clinical trials are not based on precision medicine because of the lack of biomarkers to assess the response. Therefore, the response rate of most current clinical trials is less than 40% [4,6,7]. Identifying drug-specific biomarkers is a necessity and a first step toward overcoming this challenge. It has become imperative to discover biomarkers that can identify the optimal target population and predict the therapeutic response of the drug at a preclinical stage.
Recently, two new strategies have been proposed for clinical trials in personalized medicine. The first trial design, called the basket trial, is to determine drugs that are effective against various types of cancers, and the second, called the umbrella trial, is to determine the efficacy of the various drugs for a specific type of disease condition [8]. Therefore, this study was conducted in two stages to find a drug-specific biomarker for a dipeptidyl peptidase (DPP)-4 inhibitor. First, we attempted to find the optimal target population by using the best of three kinds of animal NAFLD models. In the second step, we tried to find a biomarker that can predict efficacy in the optimal population among specific NAFLD phenotypes. The development of biomarkers that can predict treatment response before large-scale clinical trials could increase the success rate and reduce the sample size of trials, thereby reducing the enormous costs. Liver disease is a metabolic disease that is closely related to type 2 diabetes [9,10]. DPP-4 inhibitors, commonly used to treat type 2 diabetes, potentiate their effect on glycemic control by increasing levels of glucagon like peptide-1, a substrate of DPP-4, and are often proposed as a candidate for the treatment of NAFLD. The liver is the highest DPP-4 expressing organ, and serum DPP-4 levels are significantly increased in patients with NAFLD and nonalcoholic steatohepatitis (NASH) [11,12]. In addition, DPP-4 inhibitors can improve steatosis in a mouse model of diet-induced NAFLD [13-15]. However, the mechanism by which antidiabetic drugs directly ameliorate NAFLD/NASH is unclear. Therefore, we aimed to identify the optimal target population or phenotype of patients for DPP-4 inhibitors in NAFLD treatment and to identify a novel biomarker.
MATERIALS AND METHODS
Detailed experimental methods are described in the Supplementary Materials.
Animals
Six-week-old C57BL/6N wild-type male mice (18ŌĆō20 g) were purchased from Orient Bio Inc. (Orient Animal Laboratory, Seoul, Korea; study I). Six-week-old C57BL/6J wild-type male mice (18ŌĆō20 g) were purchased from the Jackson Laboratory (Bar Harbor, ME, USA; study II, III). The experiment was conducted after a 1-week acclimatization period. The animals were kept in a specific pathogen-free room in which temperature and humidity were maintained at 23┬░C┬▒2┬░C and 60%┬▒10%, respectively, under a 12-hour light/12-hour dark cycle. All experimental procedures were approved by the Hanyang Institutional Animal Care and Use Committee (study I: HY-IACUC-19-0010, study II: HY-IACUC-20-0017, and study III: HY-IACUC-21-0043).
Modified basket study design in NAFLD animal models: exploration study (study I)
Three diet-induced NAFLD models were used to modify the basket trial. A 60 kcal% high-fat diet (HFD; Research Diet #D12492), high-cholesterol Western diet (WD; Research Diet #D12079B), and methionine choline-deficient diet (MCD; Research Diet # A02082002BR) were purchased from Research Diets Inc. (New Brunswick, NJ, USA). The HFD, WD, and MCD were assigned to each group of 10 animals. The treatment group (n=5) received 200 mg/kg (200 ╬╝L) of evogliptin (Dong-A ST Co., Ltd., Seoul, Korea) dissolved in 0.5% (w/v) methylcellulose administered orally each day for 8 weeks. The control group (n=5) received 200 ╬╝L of 0.5% (w/v) methylcellulose administered orally for 8 weeks. All mice were sacrificed 8 weeks after the first administration of the DPP-4 inhibitor, and their liver tissues and blood were harvested in the laboratory.
Pre-study liver biopsy and randomization
After administration of the HFD and WD (6 weeks in the case of MCD) for 16 weeks, all animals were randomized according to the NAFLD activity score (NAS) using a pre-study liver biopsy. The pre-study liver biopsy was performed according to a previous protocol [16]. Zoletil (Virbac Laboratories, Carros, France; 40 mg/kg) and Rompun (Bayer Korea, Seoul, Korea; 5 mg/kg) were used to anesthetize the animals via intraperitoneal injection. After an abdominal midline incision (less than 1 cm), the liver was exposed with a cotton swab and a portion was excised. After surgery, the animals were kept under a heating lamp to keep them warm and treated with tetracycline (87,128; Sigma-Aldrich, Deisenhofen, Germany) for 3 days. NAS evaluation was performed after hematoxylin and eosin staining of the liver tissue, and only animals with biopsy-proven fatty livers (NAS Ōēź3 points) were selected.
Validation study using the suggested biomarker (study II)
A validation study was performed only for the HFD group. After administration of the HFD for 20 weeks, a preliminary liver biopsy was performed. The hepatic insulin-like growth factor binding protein 1 (Igfbp-1) expression was evaluated in a preliminary liver biopsy sample. The control (n=3) and evogliptin (200 mg/kg) treatment groups were randomized according to the NAS and the degree of Igfbp-1 expression. The evogliptin treatment groups were divided into high (n=5) and low (n = 6) Igfbp-1 groups. All mice were sacrificed 1 day after the last dose of the drug.
Biomarker association in the liver and serum: a developmental study using the suggested biomarker (study III)
A developmental study was performed in a group fed an L-amino acid diet with 60 kcal% fat with 0.1% methionine and no added choline (choline-deficient high fat; CDHF). The CDHF (Research Diet #A06071302) was purchased from Research Diets, Inc. The CDHF control and the CDHF+linagliptin groups consisted of 10 and 20 mice, respectively. Linagliptin (Yuhan Corporation, Yongin, Korea). was mixed with the feed at a concentration of 1 mg/kg and administered for 10 weeks. The blood was first collected 14 weeks after the ingestion of the CDHF diet; linagliptin was then administered and blood was collected again 10 weeks later.
Definition of a responder and non-responder
If the NAS decreased by more than 1 point at the end of treatment compared to that in the pre-study liver biopsy, the mouse was defined as a responder, whereas a non-responder did not show a reduction in the NAS at the end of the treatment compared to baseline NAS.
Luminex multiplex assay
At the end of the experiment, mouse serum was harvested and stored at ŌłÆ80┬░C for Luminex multiplex analysis. Multiplex analysis was performed by personnel at Woongbee Meditech Biotechnology Inc. (Seoul, Korea), and serum levels of mouse insulin-like growth factor-1, insulin-like growth factor-binding protein (IGFBP)-1, IGFBP-3, and human IGFBP-1 were determined. Standard curves for each cytokine kit (LXSAMSM-01, LXSAMSM-02, and LXSAHM-01; R&D Systems, Minneapolis, MN, USA) were generated using the reference cytokine concentrations provided by the manufacturer.
RESULTS
Characteristics of the modified basket trial design in the NAFLD animal model
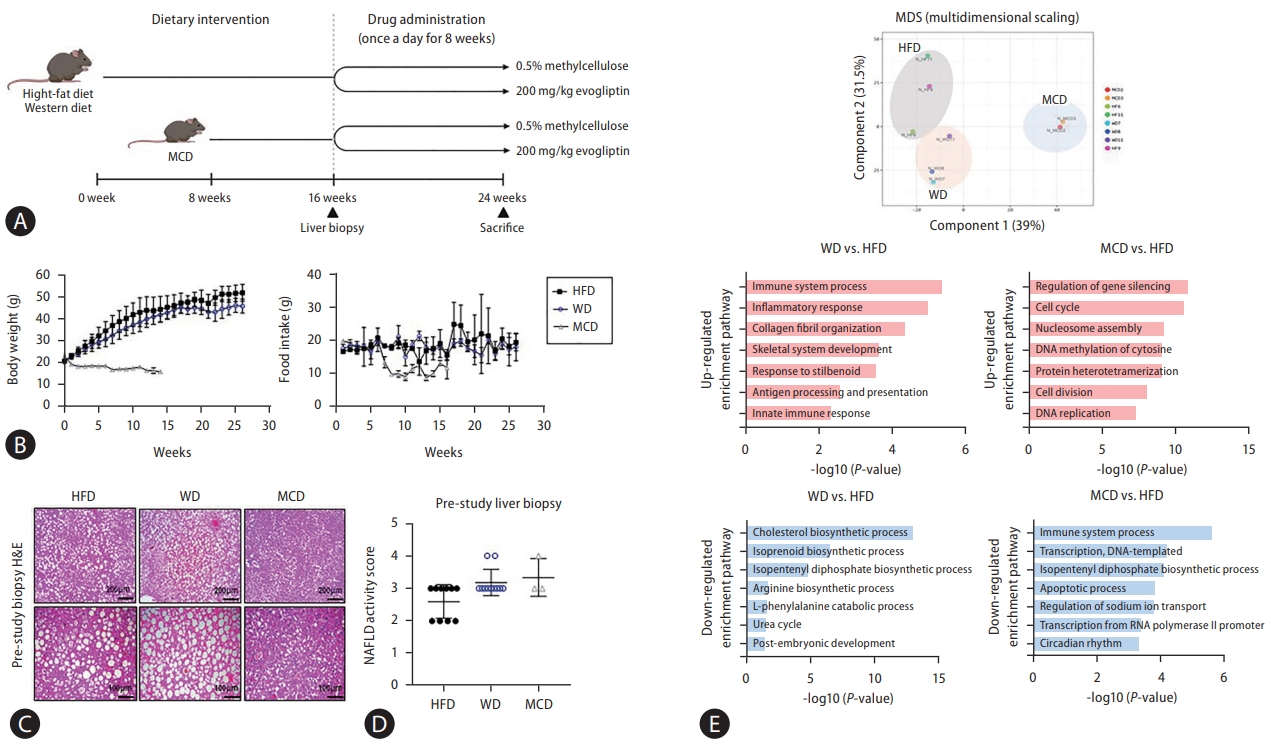
Three different NAFLD models (basket study design; HFD, MCD, and WD models) were used, and a pre-study liver biopsy was performed (Fig. 1A). There was no change in the body weight and food intake in the mice fed an HFD or WD, body weight and food intake were lower in those fed the MCD (Fig. 1B). A liver biopsy was performed before the mice received DPP-4 inhibitors, and only animals with a NAS of Ōēź3 were selected (Fig. 1C, D). RNA transcriptome data were analyzed from liver biopsies before DPP-4 inhibitor treatment. Multidimensional scaling data showed different patterns for the three NAFLD models. An analysis conducted with the Database for Annotation, Visualization, and Integrated Discovery (DAVID) program (version 6.8; http://david.abcc.ncifcrf.gov/) indicated that the decreased liver regeneration capacity of MCD compared to HFD was associated with an increase in the Usp-2 gene, which decreased cellular adenosine triphosphate levels [17]. Considering that the MCD did not exhibit insulin sensitivity and had low lipid synthesis, genes that were downregulated with the MCD compared to the HFD were those in the Fos gene family (Ptgs2, Myc, JunB, Socs3), which are related to the immune system and response to cytokines [18]. In mice fed the WD, levels of pro-inflammatory cytokines (Ccr2, Ccl6, tumor necrosis factor) and collagen fibril organization (Col1a1, Col1a2, Col3a1) were increased compared to those fed the HFD. HFD specifically led to an increased expression of genes related to cholesterol synthesis pathways (Mvk, Pmvk, Mvd) compared to WD (Fig. 1E, Supplementary Fig. 1).
Defining the DPP-4 inhibitor target population from the NAFLD basket trial
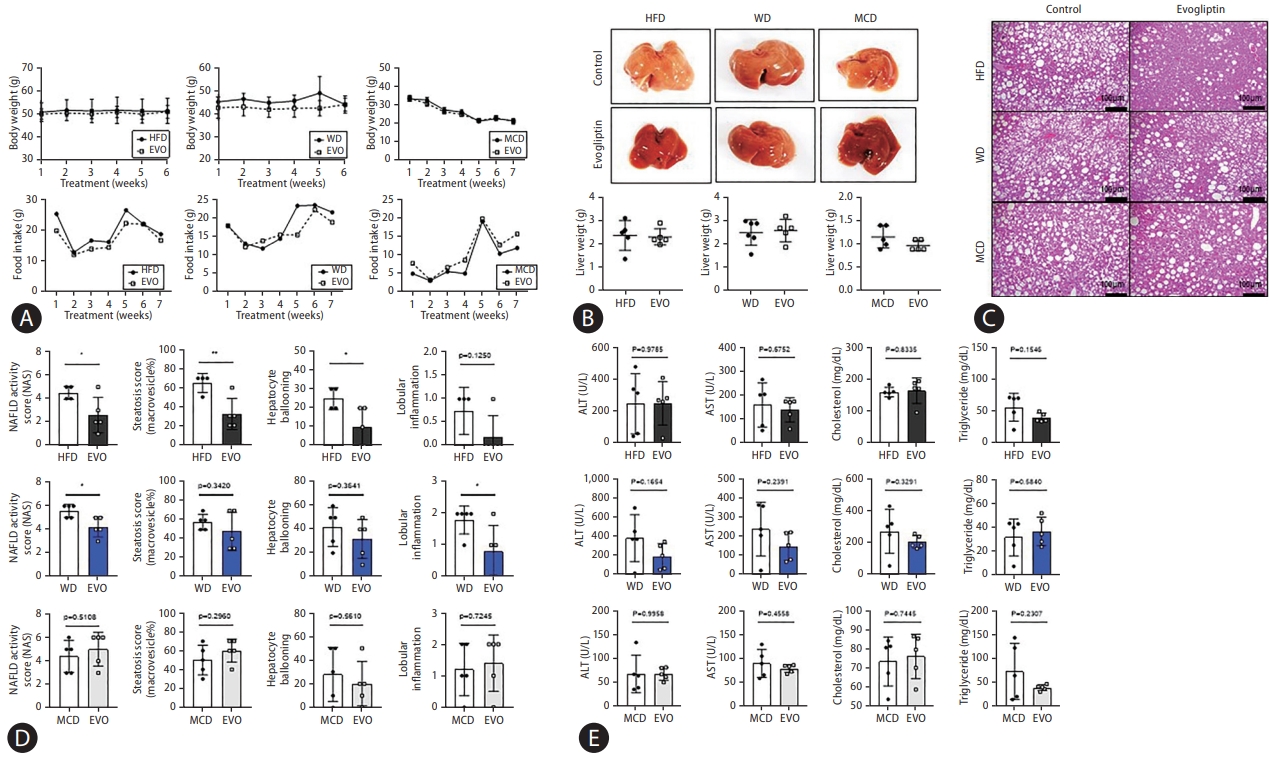
There were no differences in body weight, food intake, and liver weight between control and evogliptin-treated groups in the three NAFLD mouse models (Fig. 2A, B). Hepatic steatosis, hepatocyte ballooning, and NAS were significantly reduced in the HFD. Total NAS and liver inflammation were significantly reduced in the WD, but not in the MCD. The overall response rate to evogliptin was 19.3% in the modified basket NAFLD animal study. The NAS improvement rates were 42%, 25%, and 0% in the HFD, WD, and MCD, respectively (Fig. 2C, D, Table 1). There was no significant difference between the control and evogliptin-treated groups in the three models (Fig. 2E). The quantitative collagen proportional area decreased in the HFD and WD but not in the MCD (Fig. 3A). In addition, messenger RNA (mRNA) expression for fibrosis markers (╬▒-smooth muscle actin [╬▒-SMA], Col1a1, Timp-1) was lower in the evogliptin-treated groups, but not in mice fed the MCD (Fig. 3B). Moreover, mRNA expression of hepatic lipogenesis genes Pparg was decreased in the HFD and WD evogliptin-treated groups compared to the control group. We also found that mRNA expression of very low density lipoprotein secretion markers in the MCD evogliptin-treated group revealed a decrease in Scd-1 compared to the control group but increased expression of ApoB. The expression of the ╬▒-SMA protein decreased in the HFD and WD evogliptin-treated groups compared to the control group (Fig. 3C). The plasma insulin concentration was lower in mice fed the MCD (159.6┬▒4.62) compared with those fed the HFD (181.2┬▒5.92) and WD (174.67┬▒5.06). The receiver operating characteristic curve of the insulin tolerance test was not different in the HFD and WD evogliptin-treated groups compared to the control group (Fig. 3D).
Pre-study hepatic Igfbp-1 expression was high in the responder group
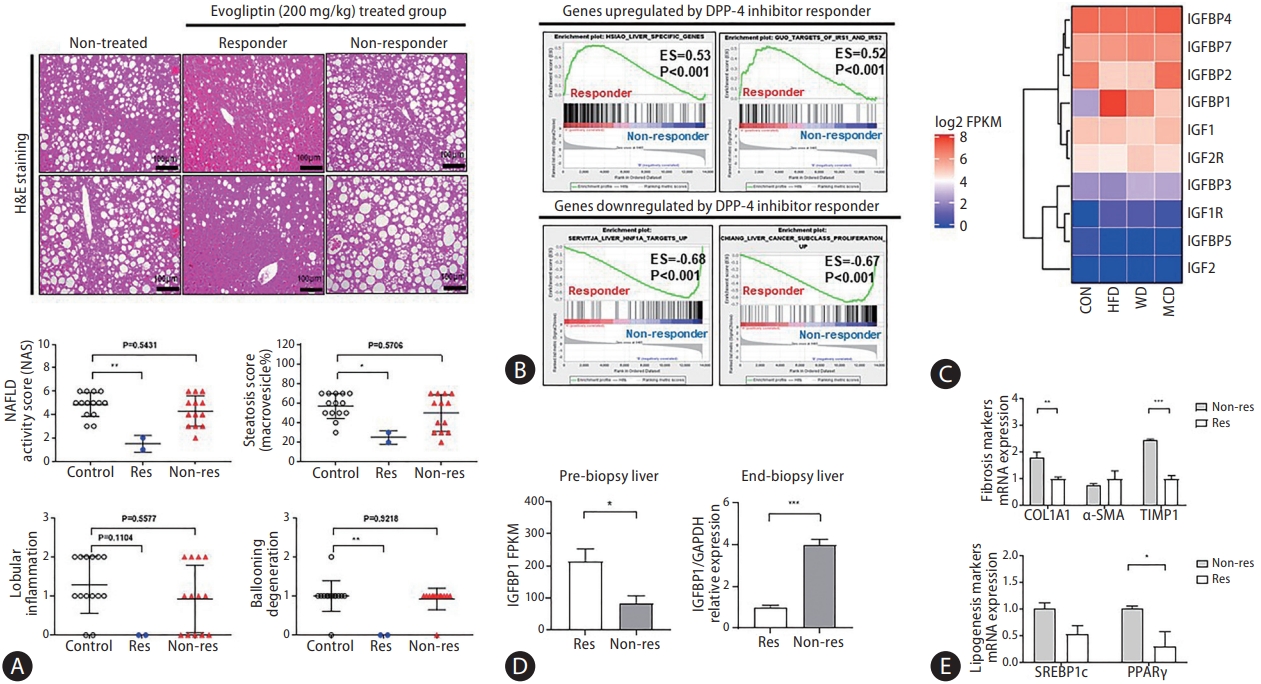
The response and non-response groups were divided according to changes in NAS (Fig. 4A). Responders were defined as those with a NAS that decreased by more than 1 point at the end of treatment compared to the pre-study liver biopsy. Transcriptome analysis was performed for biomarker discovery using pre-study liver biopsy samples from responders and non-responders. Gene set enrichment analysis showed elevated expression of the Igfbp-1-related pathway in the responders compared to that in the non-responders in the pre-study liver biopsy (Fig. 4B, Supplementary Table 1). Moreover, the expression level of Igfbp-1 (log2 fragments per kilobase of transcript per million) was significantly increased with the NAFLD-induced diet (HFD, 7.70; WD, 6.27; MCD, 4.97) compared to the normal chow diet (2.56). Hepatic Igfbp-1 expression was higher in the HFD and responder groups (Fig. 4C, Supplementary Fig. 2).
Hepatic Igfbp-1 expression was lower in the responder group at the end of treatment
Hepatic Igfbp-1 expression was compared between responders and non-responders at the end-study liver biopsy. Hepatic Igfbp-1 expression was higher in responders than in non-responders in the pre-study liver biopsy. However, hepatic Igfbp-1 expression was lower in responders than in nonresponders at the end-study liver biopsy (Fig. 4D). The expression of hepatic fibrosis markers was also lower in responders than in non-responders (Fig. 4E).
Validation study for DPP-4 inhibitor-specific biomarker in the NAFLD model
The validation study for DPP-4 inhibitor-specific biomarkers was performed in an additional HFD study. A pre-study liver biopsy was performed at 20 weeks. The HFD was divided into two groups according to hepatic Igfbp-1 expression (high vs. low Igfbp-1) before the evogliptin treatment (Fig. 5A, Supplementary Fig. 3A). Liver and body weights did not differ between the high and low Igfbp-1 groups after evogliptin treatment (Supplementary Fig. 3B). The total NAS was lower in the high Igfbp-1 group than in the low Igfbp-1 group at the end-study liver biopsy (2.8 vs. 5.2, P<0.05) (Fig. 5B, Supplementary Table 2). The levels of hepatic collagen deposition and ╬▒-SMA expression were lower in the high Igfbp-1 group than in the low Igfbp-1 group (Fig. 5C). The levels of the inflammatory marker interleukin-6 receptor were significantly decreased in both low Igfbp-1 (P=0.0278) and high Igfbp-1 (P=0.0013) groups compared with the HFD control group. Igfbp-1 expression was lower in the high Igfbp-1 group (P=0.0368) than in the HFD control group. The serum levels of alanine aminotransferase (ALT) and aspartate aminotransferase were significantly lower in the evogliptin-treated group than in the HFD control group (Supplementary Fig. 3C), but there was no difference according to Igfbp-1 expression level (Supplementary Fig. 3D). In mRNA expression analysis, fibrosis markers ╬▒-SMA, Col1a1, and Timp-1 were significantly lower in the evogliptin-treated group than in the HFD control group (Supplementary Fig. 3E). In addition, mRNA expression for the fibrosis markers ╬▒-SMA and Col1a1 was lower in the high Igfbp-1 group than in the low Igfbp-1 group (Fig. 5D). Additionally, we analyzed the levels of beta-oxidation markers (Acox1, Cpt1a) and lipogenesis markers (Fas, Scd-1). As a result, Fas increased in the high Igfbp-1 group, and Scd-1 was decreased in both the low and high Igfbp-1 groups. Protein expression of FN-1 and p-GSK3╬▓ were also lower in the high Igfbp-1 group than in the low Igfbp-1 group (Fig. 5E). Analysis of the protein expression levels of DPP-4/CD26 revealed decreases in the high Igfbp-1 group compared to the HFD control group (Fig. 5F).
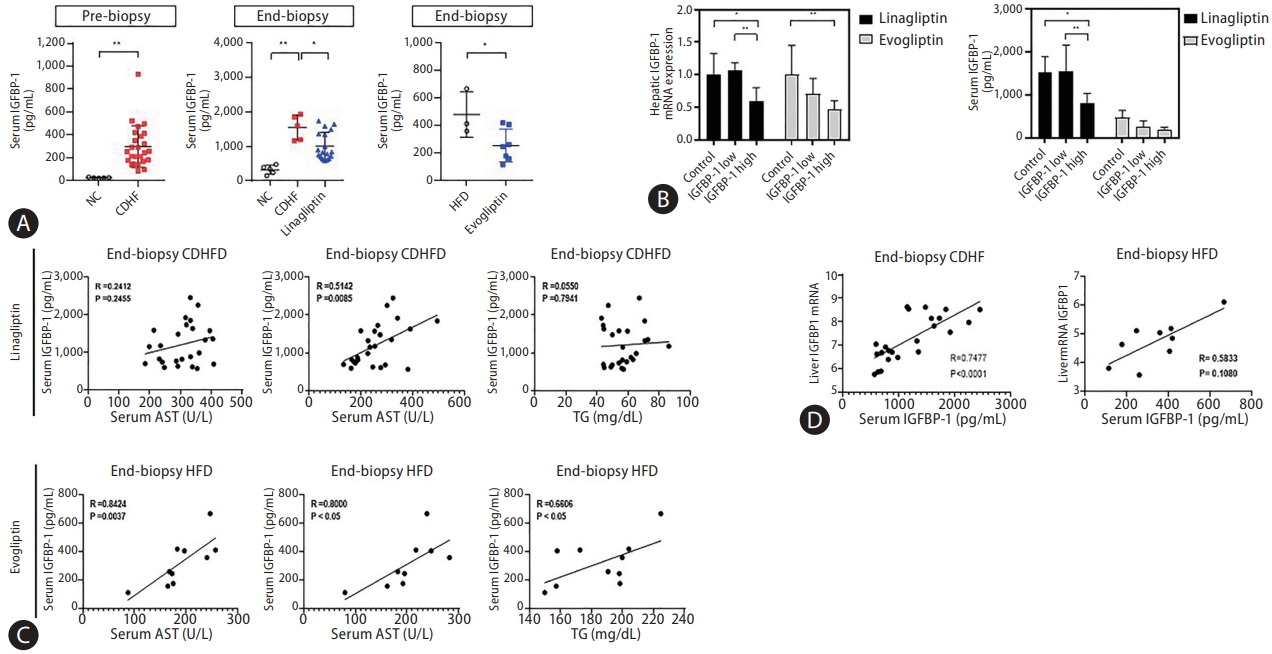
Association between the serum and hepatic IGFBP-1 expression
The correlation between the serum IGFBP-1 (sIGFBP-1) concentration and hepatic IGFBP-1 level was evaluated. Levels of sIGFBP-1 increased in the NAFLD patients compared to healthy controls. In addition, sIGFBP-1 increased in the NAFLD mouse model and decreased after treatment with DPP-4 inhibitors (Fig. 6A, Supplementary Fig. 4). Interestingly, hepatic Igfbp-1 expression and sIGFBP-1 concentration decreased after DPP-4 inhibitors treatment only in the high Igfbp-1 group (Fig. 6B). Changes in serum IGFBP-3 (sIGFBP-3) and serum IGF-1 (sIGF-1) levels were not significant in the NAFLD mouse model or after DPP-4 inhibitor treatment (Supplementary Fig. 5A). Levels of sIGFBP-1 were positively correlated with ALT levels before and after DPP-4 inhibitor treatment (Fig. 6C, Supplementary Fig. 5B). Hepatic mRNA Igfbp-1 expression also showed a positive correlation with sIGFBP-1 levels (Fig. 6D). There was no significant difference in the correlation analysis results between liver Igfbp-1 and sIGFBP-3 or sIGF-1 in various DPP-4 inhibitor studies (Supplementary Fig. 5C). In addition, in an analysis of the effect of the DPP-4 inhibitor according to sIGFBP-1 or sIGFBP-3 before administration, NAS was significantly decreased in the high sIGFBP-1 group (Supplementary Table 3). The correlation between blood IGFBP-1 concentration and DPP-4 inhibitors in the NAFLD mouse model was verified through paired and serum analyses before and after drug treatment. The concentration of sIGFBP-1 was confirmed to be positively correlated with the expression of IGFBP-1 in the liver.
DISCUSSION
The overall response rate to DPP-4 inhibitors was 19.0% in the modified basket NAFLD study. Hepatic Igfbp-1 expression was higher in the responders than in the non-responders; however, after DPP-4 inhibitor treatment, it was lower in the responders. The overall response rate to DPP-4 inhibitors was 87% in patients with high Igfbp-1 levels at the pre-study stage. Thus, high Igfbp-1 levels at the pre-study stage may be a DPP-4 inhibitor-specific biomarker for NAFLD treatment.
The strengths of this study are as follows. First, we modified the basket study design to include an animal model for the first time. The basket trial design was applied to customize treatment in specific cancer patients [19,20]. This new study design was proposed to develop drug-specific biomarkers for various drugs and to discover an optimal target group. To date, the criteria for selecting animal models for preclinical studies of NAFLD have been ambiguous. Our proposed basket NAFLD animal study suggests an optimal target group for NAFLD and demonstrates a more objective efficacy using an unbiased setting. Second, a pre-study liver biopsy was performed before drug administration, and randomization was performed according to histologic severity. We believe that this method provides a high level of evidence on the response to treatment. A previous study reported heterogeneity despite the induction of NAFLD in mice with the same diet and genetic background [16]. Therefore, we tried to obtain more objective results by excluding animals that did not develop fatty liver, as determined in a pre-study liver biopsy, which can stratify the degree of fatty liver in each group. Third, we validated the proposed biomarker by using an additional validation study to verify the predictive performance of the biomarker proposed in the modified basket study.
Currently, there are approximately 11 DPP-4 inhibitors in the global market. Despite slight differences in efficacy, DPP-4 inhibitors can lower blood sugar levels. However, their effectiveness in the treatment of NAFLD has not yet been established [21]. Data on DPP-4 inhibitors in patients with NAFLD are limited. To date, only four clinical studies have been published; these were based on MRI results, and the improvement rate of intrahepatic fatty liver was 8% [22-25]. However, there is no liver histology-based clinical data regarding DPP4 inhibitors in NAFLD. In our study, the mean response rate of DPP-4 inhibitors in the basket NAFLD animal model was 19%. The response rates of the three NAFLD animal models were different for each model (25%, 42%, and 0% in the WD, HFD, and MCD models, respectively). When we applied a new biomarker (IGFBP-1), the response rate of the DPP-4 inhibitor was 83% in the high Igfbp-1 group. Although we demonstrated that the expression of intrahepatic Igfbp-1 showed a good correlation with sIGFBP-1 levels, this study did not suggest a cut-off point for IGFBP-1 that could indicate a good response.
In this study, the high expression of Igfbp-1 in a liver biopsy increased the response rate, and this expression decreased in the liver and serum after the administration of a DPP-4 inhibitor. IGFBP-1 is associated with insulin resistance and predicts the development of type 2 diabetes [26]. Given that DPP-4 inhibitors are used in the management of diabetes, it seems logical that IGFBP-1 may predict the treatment response to DPP-4 inhibitors. Therefore, hepatic Igfbp-1 may be involved in the hepatic insulin signaling pathway. Hepatic Igfbp-1 mRNA expression is inversely associated with glycemia and insulin resistance in patients with NAFLD [27]. Interestingly, the hepatic expression levels of Irs-1, Irs-2 and IGFBPs were higher in the HFD model than in the other diet models. In addition, the response to the DPP-4 inhibitor was also the best in the HFD model in our study.
Our study has some limitations. We confirmed that the treatment response was high when hepatic Igfbp-1 expression was high before treatment. However, there is no clear cutoff for high and low levels of hepatic Igfbp-1. We could not suggest a method for quantifying the expression level of Igfbp-1 in the liver. We observed a positive correlation between sIGFBP-1 levels and Igfbp-1 expression in the liver. However, the correlation was not sufficient to replace the hepatic Igfbp-1 level; therefore, it is difficult to predict treatment response using the sIGFBP-1 level. Additional research is required to generalize the above data to all DPP-4 inhibitors.
In conclusion, the overall response rate to DPP-4 inhibitors was 19% in this basket NAFLD animal model study. The DPP4 inhibitor response was higher in the HFD model than in the other types of NAFLD models, and the response rate increased to 83% in the high Igfbp-1 HFD model. Based on these results, we suggest that the high expression of Igfbp-1 before DPP-4 inhibitor treatment increases the treatment response rate in a NAFLD model.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Supplement1
Supplement1 Print
Print





