


INTRODUCTION
Hepatocellular carcinoma (HCC) is the most common primary liver cancer in adults and the second leading cause of cancer-related death worldwide [1]. HCC occurs primarily in patients with chronic liver disease with various etiologies such as viral hepatitis, alcohol-induced liver disease, and nonalcoholic steatohepatitis [2]. As curative treatment options for HCC including surgical resection, liver transplantation, and ablation treatments are effective for early-stage HCC, timely diagnosis and early intervention are crucial in the management of patients with HCC [3]. Considering that HCC can be diagnosed noninvasively using imaging tests without confirmatory biopsy [4] and that imaging-based staging is essential for treatment selection, imaging plays critical role in management of HCC.
In order to standardize the acquisition, interpretation, and reporting of liver imaging examinations, several scientific organizations have proposed imaging-based diagnostic systems for surveillance, diagnosis, staging, treatment, and monitoring of treatment response of HCC [5,6]. The designs of these HCC imaging systems have varied between geographic areas so as to address different target populations, resources, and treatment practices [5]. Despite these regional variations, HCC guidelines with imagingbased surveillance and diagnostic components have continued to improve the consistency and standardization of the acquisition, interpretation, and reporting of liver examinations [5,7]. These guidelines have also been continually updated to reflect the most recent radiological and technological advances, as well as our better understanding of HCC pathophysiology. In 2017, the Asian Pacific Association for the Study of the Liver (APASL) practice guidelines have been updated [8]. The Liver Imaging Reporting and Data System (LI-RADS) endorsed by the American College of Radiology, have been updated two years in a row, in 2017 [9] and 2018 [10]. In 2018, American Association for the Study of Liver Diseases (AASLD) âwhich released two distinct documents in the same year: HCC practice guidelines and practice guidance documents in the same yearâ [4,11] integrated LI-RADS version 2018 into their HCC clinical practice guidance document; European Association for the Study of the Liver (EASL) [12] updated their clinical practice guidelines for the management of HCC; and Korean Liver Cancer Association-National Cancer Center (KLCA-NCC) released their guidelines v 2018 in Korean [13] and the English version is expected to be published soon.
The purpose of this review article is to synthesize and critically appraise the currently published imaging-based diagnostic systems endorsed by the five major societies (KLCA-NCC, APASL, AASLD, LI-RADS, EASL) for the noninvasive diagnosis of HCC and to address some limitations of current systems. Similar to the HCC diagnostic guidelines reviews by Cruite et al. in 2013 [14], we converted the display from an algorithmic format of diagnostic systems to lists, while respecting and maintaining the original content in Tables 1 and 2.
SURVEILLANCE
Summaries of five HCC surveillance guidelines are provided in Table 1.
Target population for surveillance
All current guidelines recommend HCC surveillance in patients with liver cirrhosis or other risk factors for developing HCC. However, target populations differ in detail according to the guidelines. For example, KLCA-NCC include chronic HCV carrier whereas AASLD, EASL and APASL include cirrhotic patients with HCV [4,8,11,12]. Ultrasound LI-RADS v 2017 [15] defers to regional HCC clinical practice guidelines for enrollment of adults with cirrhosis of any etiology and chronic hepatitis B or chronic hepatitis C viral infection even in the absence of cirrhosis.
Tests for surveillance
Ultrasound every 6 months is universally recommended for HCC surveillance in all guidelines. However, KLCA-NCC and APASL [8] surveillance recommendations differ in that they utilize alpha-fetoprotein (AFP) as a tumor marker for surveillance in combination with the ultrasound, whereas use of AFP for surveillance is optional as per AASLD [4] and LI-RADS guidelines [15], and not recommended by EASL due to suboptimal cost-effectiveness for routine surveillance of early HCC [12]. AFP and ultrasound have imperfect sensitivity, but may play complementary roles when combined [16]. According to previous meta-analyses by Singal et al. [17] and Tzartzeva et al. [18], the sensitivity for detection of HCC using a combination of ultrasound and AFP is higher than that of ultrasound alone (respectively: 70% vs. 63% [P =0.65] [17], 63% vs. 45% [P =0.002]) [18]. The differences in the surveillance test among guidelines may be due to the fact that the efficacy of the surveillance method can vary depending on the thresholds and the incidence of HCC in a given region. In North America and Europe, where the prevalence is relatively low, only ultrasound is recommended as a screening method, but in Asia, including Korea, where the prevalence of HCC is high, it is recommended to perform an ultrasound and AFP measurement combined.
Also, EASL further specifies ultrasound within 4 months when a nodule smaller than 1 cm has been detected, and EASL, AASLD, and KLCA-NCC recommend consideration of computed tomography (CT) or magnetic resonance imaging (MRI) for surveillance in select patients with a high likelihood of having an inadequate ultrasound or if ultrasound is attempted but inadequate (for example due to obesity, chest wall deformity, or intestinal gas).
IMAGING-BASED DIAGNOSIS
Summaries of five diagnostic and staging guidelines are provided in Table 2.
Target population for diagnosis
LI-RADS defines different patient populations for surveillance and diagnosis. For the diagnosis of HCC, LI-RADS applies diagnostic imaging for HCC to positive surveillance ultrasound examinations or to incidental discovery of observations in patients at high risk for the development of HCC. More specifically, LI-RADS applies in patients at high risk for HCC, namely those with cirrhosis, chronic hepatitis B viral infection or current/prior HCC, including adult liver transplant candidates and recipients posttransplant, but does not apply to pediatric patients and cirrhosis due to vascular disorder or congenital hepatic fibrosis [19]. Other systems (AASLD, EASL, KLCA-NCC, and APASL) generally begin the diagnostic algorithm for patients with a positive screening/surveillance test. Additionally, AASLD and APASL recommend initiation of the diagnostic imaging in patients with clinical suspicion of HCC.
The differences in patient selection among guidelines are inevitable because of national and regional variations in incidence of HCC or major risk factors for HCC. The different definitions of target population affect the pre-test probability of disease and the positive and negative predictive value of tests [5].
Diagnostic imaging modality
All five current systems include recommendations for multiphase CT or MRI with extracellular contrast agents (ECA) or hepatobiliary contrast agents (HBA)-enhanced MRI as first-line diagnostic imaging modalities. Of note, all guidelines except APASL do not recommend one MRI contrast agent type over the other.
HBA include two gadolinium-based contrast agents: gadoxetate disodium (gadoxetic acid or Gd-EOB-DTPA) and gadobenate dimeglumine (Gd-BOPTA), which both have dual properties of conventional extracellular and HBA. Both agents show hepatocellular uptake via organic-anion-transporting polypeptide (OATP) transporters and biliary excretion via multidrug resistance-associated protein (MRP2) transporters. However, 50% of gadoxetate disodium compared to 5% of gadobenate dimeglumine is eliminated by biliary excretion. In general, a persistent, strong enhancement of the background liver via cellular uptake can be observed during the hepatobiliary phase (HBP) whereas premalignant or malignant hepatocellular tumors having diminished or absent transporter function show hypoenhancement. These changes in transporters of hepatocytes is shown earlier than the hemodynamic changes in hepatocarcinogenesis [20,21]. Furthermore, the improved lesion-to-liver contrast during the HBP leads to higher sensitivity for the detection of HCCs than CT or MRI using extracellular contrast media [22]. To acknowledge the benefits of HBAenhanced MRI, all guidelines include MRI with HBA in addition to dynamic CT or MRI with ECA as first-line diagnostic imaging tests.
For contrast-enhanced ultrasound (CEUS), LI-RADS also provides guidance for the performance and interpretation of CEUS. However, LI-RADS does not advocate for any particular imaging modality (CEUS, CT or MRI) over the other as first-line diagnostic imaging [23]. Because of moderate evidence [12], the challenges of characterizing multiple nodules and comparing with CT or MRI examinations, EASL provided a weak recommendation in favor of using CEUS for the diagnosis of HCC, whereas KLCA-NCC and APASL recommend CEUS as second-line modality when initial first-line diagnostic imaging is inconclusive. However, AASLD has not endorsed CEUS as a diagnostic imaging for HCC.
As of now, most guidelines recommend CEUS as a secondary imaging modality, most likely due to its several potential weaknesses, i.e., the lower detection rate for washout of HCCs than with CT or MRI [24-26], limited capability of staging [24,25], limited performance in some patients with a poor sonic window or advanced cirrhosis, and lack of availability except in expert centers [11]. It is controversial whether CEUS can make a specific diagnosis of HCC due to the potential risk of a misdiagnosis in the case of massforming cholangiocarcinomas (CCs) which manifest global arterial phase hyperenhancement (APHE) followed by washout at CEUS, leading to a misdiagnosis of HCC in approximately 50% of the cases. Many studies performed over the past two have proven the ability of CEUS to differentiate between HCC and CCs with different APHE characteristics, timing, and degree of washout. HCCs at CEUS showed APHE followed by late (>60 seconds) washout of a mild degree [27,28], whereas many CCs at CEUS showed APHE followed by early (<60 seconds) marked washout [29-32]. Recently, a large retrospective study [33] including more than 1,000 lesions in cirrhosis, has shown that these new refined criteria of the typical HCC pattern had a positive predictive value of almost 99% for HCCs and a positive likelihood ratio of 15.5, with no false-positive diagnoses owing to CCs. In another recent prospective multicenter study [34], albeit the application of the refined criteria of CEUS was unclear, CEUS showed a specificity of 92.9% vs. 76.8% and 83.2% in 10-20 mm nodules for CT and MRI, respectively. Furthermore, after a first inconclusive CT or MRI, CEUS as a second imaging technique showed the highest specificity with only a slight drop in sensitivity for 10-20 mm nodules and the highest sensitivity and specificity for 20-30 mm nodules [34].
There are two types of contrast agents for CEUS: pure bloodpool contrast agents and postvascular phase agents taken up by Kupffer and/or reticuloendothelial cells. SonoVueÂŪ (sulfur hexafluoride with a phospholipid shell: Bracco SpA, Milan, Italy) and DefinityÂŪ/Luminity ÂŪ (octafluoropropane [perflutren] with a lipid shell: Lantheus Medical, Billerica, MA, USA) are common bloodpool agents while SonazoidÂŪ (perfluorobutane: GE Healthcare, Chalfont St. Giles, UK) is a postvascular phase agent. Unlike SonoVue ÂŪ or DefinityÂŪ, SonazoidÂŪ provides additional Kupffer phase images (usually 10 to 60 minutes after its injection) at which typical HCCs show hypoechogenicity, indicating a lack of contrast uptake corresponding to the lack of Kupffer cells and/or reticuloendothelial cells [35,36].
Both EASL and KLCA-NCC guidelines in 2018 recommend the use of intravascular contrast agents such as SonoVueÂŪ as a CEUS contrast agent for the diagnosis of hypervascular HCC. According to EASL and KLCA-NCC guidelines, to diagnose arterially hyperenhancing HCC with CEUS, the lesion larger than 1 cm should manifest APHE followed by late (>60 seconds after injection of the contrast agent) washout of mild degree. CEUS offers several advantages over CT/MRI including the depiction of arterial hypervascularity with high temporal resolution, and better demonstration of early washout of non-HCC malignancies and of very late washout of HCC [37]. These advantages of CEUS could result in high specificity when CEUS was added to either CT or MRI [34]. In addition, APASL recommends usage of SonazoidÂŪ for the diagnosis of non-hypervascular HCC (i.e., arterial phase iso- or hypoenhancing HCC on CT or MRI) [8]. When a non-hypervascular nodule shows hypoenhancement on HBP of gadoxetic acid-enhanced MRI, SonazoidÂŪ-enhanced ultrasonography (US) can be used as a second-line diagnostic test to diagnose HCC on the basis of APHE and/or defect
on defect on Kupffer phase. Until now, AASLD does not endorse the usage of CEUS in the HCC diagnostic algorithm [11].
Imaging criteria for arterial phase hyperenhancing HCC
Before we dive into the imaging criteria for the diagnosis of HCC, it is noteworthy that the AASLD 2018 practice guidance document incorporated CT/MRI LI-RADS categories into its diagnostic algorithm [11]. All guidelines consider the combination of APHE and washout appearance as a hallmark feature of definite HCC. There are specific differences in the definition of washout on MRI with HBA and in the size requirement for the diagnosis of definite HCC among guidelines.
When it comes to washout appearance, all guidelines require washout on either portal venous phase or delayed phase on CT/MRI with extracellular contrast agent. However, on MRI with the HBA, AASLD, EASL, and LI-RADS strictly define washout on only portal-venous phase, whereas only KLCA-NCC encompasses washout on portal, transitional and HBP. Furthermore, when there is no washout on portal venous phases on MRI with the HBA, APASL allow hypointensity on HBP as an alternative for washout after exclusion of cavernous hemangioma. Also, the Korean guideline specifically excludes marked T2 hyperintensity or targetoid appearance in the diffusion weighted image or contrast enhanced T1-weighted image when HBA is used. Regarding the size of the nodule, only APASL permits the definite diagnosis of HCC regardless of size (including subcentimeter nodules) whereas other guidelines require a minimum diameter of 10 mm as a prerequisite for definite HCC.
Enhancing capsule appearance and threshold growth constitute major imaging features of HCC in AASLD and LI-RADS. Threshold growth is defined as a âdiameter increase by at least 50% if the time interval is 6 months or lessâ [10].
Imaging criteria for arterial phase iso- or hypoenhancing HCC
All current systems heavily depend on the vascular enhancement pattern appearance for imaging-based definitive diagnosis of HCC: APHE with subsequent washout. Therefore, regarding nodules with arterial phase iso- or hypoenhancement on CT or MRI, only APASL guidelines provide criteria for a definitive diagnosis of HCC whereas other guidelines do not allow the definitive diagnosis of HCC. The APASL criteria for arterial phase iso- or hypoenhancing HCC are as follows: non-APHE nodule on CT or MRI showing HBP hypointensity on HBA-enhanced MRI and hypervascularity on subsequent CEUS with SonazoidÂŪ (defect in the Kupffer phase is not mandatory).
Imaging criteria for arterial phase iso- or hypoenhancing probable HCC
Among the five guidelines, AASLD, LI-RADS, and KLCA-NCC guidelines allow categorization of observations with arterial phase iso- or hypoenhancement as probable HCCs, whereas EASL and APASL do not allow a probable diagnosis. AASLD and LIRADS allow arterial phase iso- or hypoenhancing observations to qualify as probable HCC (designated as LI-RADS 4) with different combinations of major imaging features. For nodules with arterial phase iso- or hypoenhancement, at least one additional major feature (among nonperipheral washout, enhancing capsule or threshold growth) is required for nodules âĨ20 mm and at least two additional major features are quired for nodules <20 mm. LIRADS also permits upgrading (up to LI-RADS 4) or downgrading LI-RADS categorization with the combination of ancillary features.
KLCA-NCC also allows categorization of arterial phase iso- or hypoenhancing nodules as probable HCC depending on the combination of ancillary imaging features. For nodules âĨ1 cm in diameter with the absence of typical imaging features, the arterial phase iso- or hypoenhancing probable HCC can be diagnosed if there is at least one ancillary imaging features suggesting malignancy and at least one of those suggesting HCC appear. Ancillary imaging features suggesting malignancy include intermediate T2 hyperintensity on T2-weighted imaging, high signal intensity on diffusion-weighted imaging, and interval growth on follow-up imaging. Ancillary imaging features suggesting HCC include the presence of a capsule, mosaic appearance, nodule-in-nodule appearance, intratumoral fat, and intratumoral hemorrhage.
Diagnostic scope
The systems differ in the category of HCC. EASL guidelines address solely arterial phase hyperenhancing HCC, and two systems (AASLD and LI-RADS) address the entire spectrum of nodules and pseudolesions in patients at risk. APASL addresses not only arterial phase hyperenhancing HCC but also arterial phase iso- or hypoenhancing HCC. KLCA-NCC addresses arterial phase hyperenhancing HCC and arterial phase iso- or hypoenhancing probable HCC.
Differences between guidelines of Western societies such as AASLD, EASL and LI-RADS, and those from Eastern societies such as KLCA-NCC and APASL are attributed to several factors such as different priorities in treatment practices [5,38]. In Europe and North America, the diagnostic criteria are intentionally designed to achieve high specificity for the diagnosis of definite HCC at the expense of a decrease in sensitivity. Since patients with definite HCC may undergo liver transplantation for curative therapy based on imaging alone, high specificity was warranted to avoid falsepositive HCC diagnoses. On the other hand, in Asia, diagnostic criteria are designed to favor high sensitivity for the detection of early HCCs at the expense of a decrease in specificity [26,39]. This trade-off is intentionally made to favor early treatment and access to locoregional ablative therapies such as percutaneous ethanol injection, radiofrequency ablation, and transarterial chemoembolization for the management of patients with early-stage HCCs [4,5,26].
Staging
Guidelines differ in their perspective to tumor staging and favored treatment for each stage. The Barcelona Clinic Liver Cancer (BCLC) staging system is recommended by the AASLD and EASL guidelines. LI-RADS utilizes the radiologic T-staging system and KLCA-NCC guidelines endorse the Modified Union for International Cancer Control (mUICC) staging system.
SUMMARIES AND KEY DIFFERENTIATING FEATURES OF EACH GUIDELINE
KLCA-NCC [13]
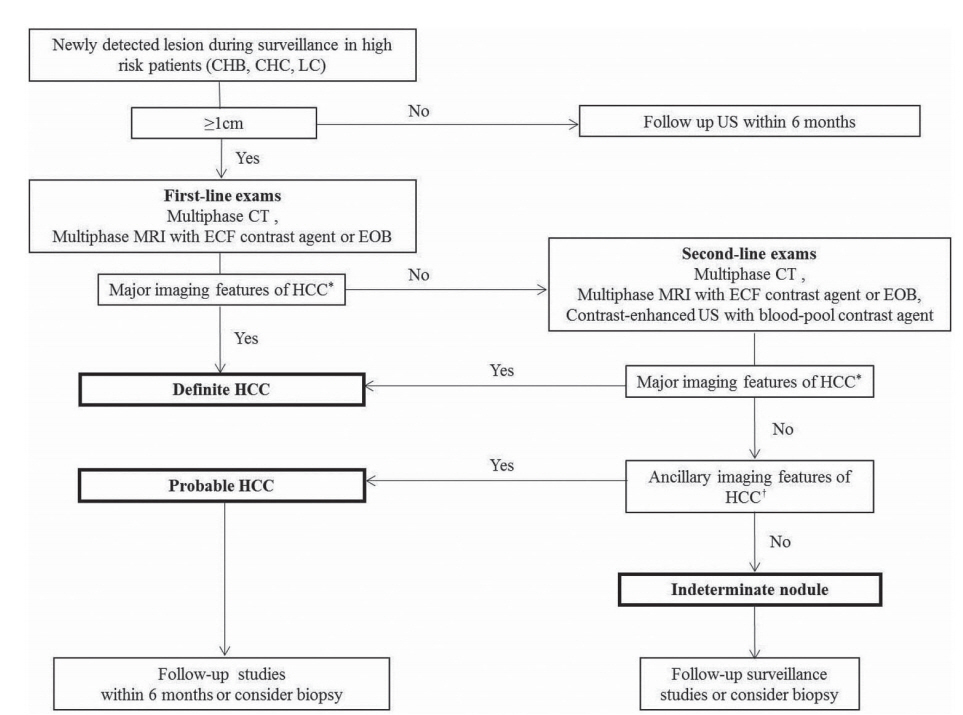
The diagnostic algorithm for surveillance and diagnosis of HCC according to KLCA-NCC is presented in Figure 1.
Target population and tests for surveillance
The KLCA-NCC guidelines v 2018 recommend ultrasound and AFP measurements every 6 months for the surveillance of HCC in patients with liver cirrhosis of varying etiology and chronic HBV or HCV carrier.
Target population and imaging modalities for diagnosis
First-line diagnostic imaging modalities including MRI with HBA in addition to dynamic CT or MRI with ECA should be performed in patients at risk for HCC with âĨ1 cm nodule on surveillance ultrasound. KLCA-NCC guidelines v 2018 permit the use of intravascular contrast agents as a CEUS contrast agent for the diagnosis of hypervascular HCC.
Imaging criteria for arterial phase hyperenhancing HCC
For observations larger than 1 cm, the combination of APHE and washout appearance is required for the diagnosis of arterial phase hyperenhancing HCC.
Regarding washout timing in HBA-enhanced MRI, the guidelines use a broad definition of âwashoutâ as hypointensity on the portal, transitional, or HBP. Of note, considering washout up to the HBP may increase its sensitivity for the diagnosis of HCC but at the cost of lowering specificity, mainly due to the pseudowashout phenomenon (i.e., caused by parenchymal enhancement rather than tumor washout per se) [40-42]. In addition, the guidelines prevent the diagnosis of HCC for any lesion that presents either a targetoid appearance on dynamic contrast enhanced images or on diffusion weighted images or marked T2 hyperintensity when using HBA. This will prevent significant loss in specificity considering that most false-positive diagnoses of HCC resulting from the use of the HBP for determining the washout appearance were made on hemangiomas, CCs, and combined hepatocellular-CCs [40]. In keeping with this perspective, Joo et al. [43] recently reported a sensitivity of 92.5% and specificity of 87.4% after broadening the definition of âwashoutâ to include hypointensity on the HBP and applying the exclusion criteria.
In order to diagnose arterially hyperenhancing HCC with CEUS, the lesion larger than 1 cm should manifest APHE followed by late (>60 seconds after injection of the contrast agent) washout of mild degree.
Imaging criteria for arterial phase iso- or hypoenhancing HCC
The guidelines do not permit the diagnosis of arterial phase isoor hypoenhancing HCC.
Imaging criteria for arterial phase iso- or hypoenhancing probable HCC
The guidelines utilize ancillary findings to diagnose probable HCCs, an approach similar to that of LI-RADS and AASLD. As a result, LI-RADS, AASLD, and KLCA-NCC use a non-binary decision algorithm covering the whole spectrum of observations seen in the liver whereas other systems including EASL and APASL use binary decisions mainly focusing on the distinction between HCCs and non HCCs.
APASL [8]
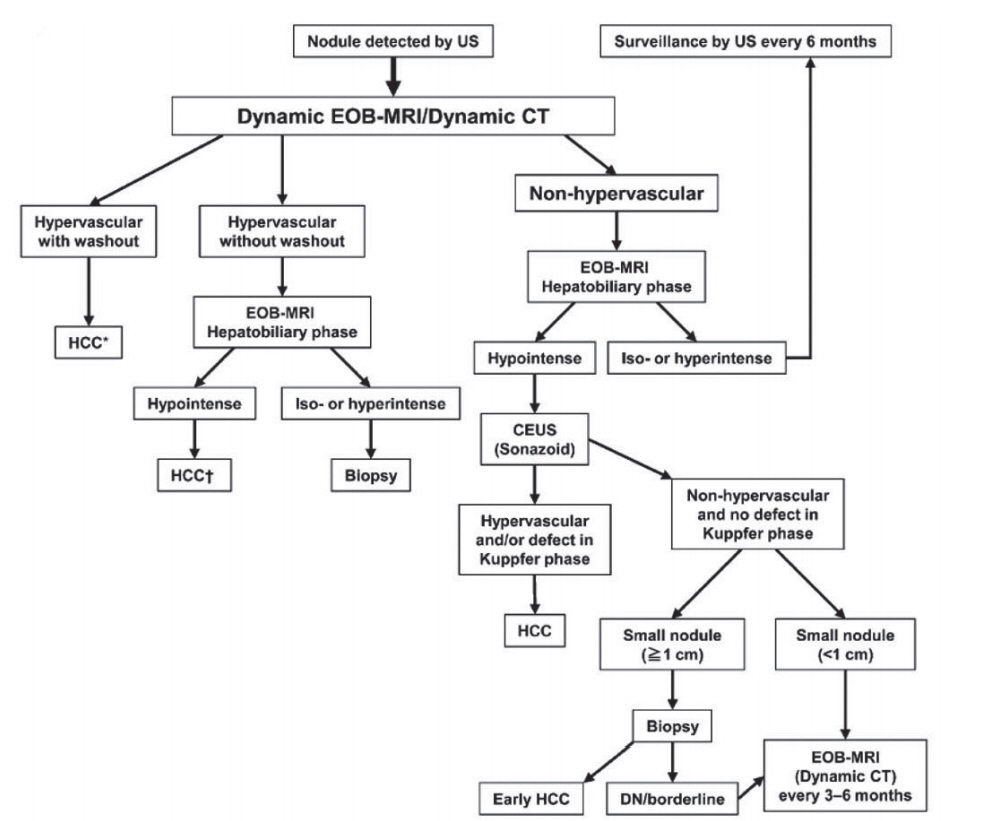
The diagnostic algorithm for HCC using multiple modalities according to APASL is presented in Figure 2.
Target population and tests for surveillance
The APASL guidelines recommend ultrasound and AFP measurements every 6 months for the surveillance of HCC in patients with liver cirrhosis of varying etiology (HBV, HCV, non-alcoholic steatohepatitis, genetic hemochromatosis, primary biliary cirrhosis, alpha-1 antitrypsin deficiency) and non-cirrhotic HBV patients (starting age slightly vary according to the ethnicity and family history of HCC).
Target population and imaging modalities for diagnosis
Regardless of the surveillance method, for patients with positive surveillance test or with clinical suspicion of HCC, the guidelines recommend the initiation of the diagnostic algorithm for HCC with first-line diagnostic imaging modalities including MRI with HBA in addition to dynamic CT or MRI with ECA. The APASL guidelines solely utilize SonazoidÂŪ as a CEUS contrast agent for the secondary imaging modality among the five guidelines discussed in this review which will be soon later discussed.
Imaging criteria for arterial phase hyperenhancing HCC
For any observations regardless of the size, the combination of APHE and washout appearance is required for the diagnosis of arterial phase hyperenhancing HCC. Regarding washout timing in HBA-enhanced MRI, APASL guidelines define âwashoutâ as hypointensity on the portal venous phase or HBP.
Imaging criteria for arterial phase iso- or hypoenhancing HCC
The guidelines allow the widest diagnostic scope for HCC among the five guidelines discussed in this review article. Only the APASL guidelines permit the diagnosis of HCC on hypovascular (i.e., with arterial phase iso- or hypoenhancement) nodules on CT or MRI, regardless of the nodule size with the usage of CEUS with SonazoidÂŪ contrast agent.
One unique feature of APASL compared to other guidelines is the usage of CEUS with SonazoidÂŪ contrast agent. Compared to CEUS with intravascular contrast agents such as SonoVueÂŪ, CEUS with SonazoidÂŪ may achieve higher sensitivity for the detection of focal hepatic lesions due to the additional Kupffer phase [44]. Furthermore, SonazoidÂŪ with defect reperfusion imaging, which consists in reinjecting SonazoidÂŪ and scanning areas showing a defect in the Kupffer phase, may improve the specificity for the diagnosis of HCC [36,45]. However, SonazoidÂŪ still has low specificity for the diagnosis of HCC because other hepatic lesions such as hemangiomas or CCs also lack Kupffer cells.
Imaging criteria for arterial phase iso- or hypoenhancing probable HCC
The guidelines do not permit the diagnosis of arterial phase isoor hypoenhancing probable HCC.
AASLD [11]
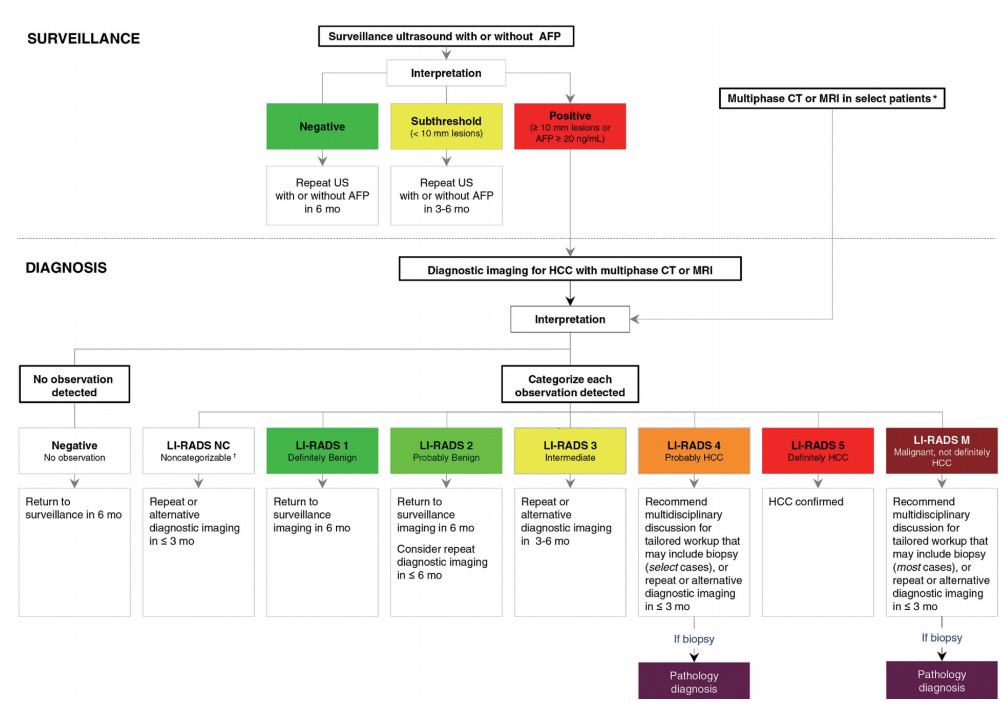
The diagnostic algorithm for surveillance and diagnosis of HCC according to AASLD is presented in Figure 3.
Target population and tests for surveillance
The AASLD guidelines recommend ultrasound with or without AFP every 6 months for the surveillance of HCC in patients with liver cirrhosis of varying etiology (HBV, HCV, primary biliary cirrhosis, genetic hemochromatosis, alpha-1 antitrypsin deficiency) and non-cirrhotic HBV patients (starting age vary according to the ethnicity and family history of HCC). CT or MRI may be utilized in select patients with a high likelihood of having an inadequate US or with performed but inadequate US examination.
Target population and imaging modalities for diagnosis
For patients with positive surveillance test or with clinical suspicion of HCC, the guidelines recommend the initiation of the diagnostic algorithm for HCC. A key change in the 2018 Practice Guidance document by the AASLD is the integration of LI-RADS into its diagnostic algorithm. AASLD recognizes that LI-RADS categories reflect the probability of HCC and of other malignancy and reflect the cumulative incidences of progression of untreated observations. For example, LI-RADS 3 observations have average possibility of 33% for HCC [46-48] with 6-15% progression into HCC or other malignancy by 24 months [49-51]. LI-RADS 4 lesion has an average probability of HCC of 80% [46-48] with 46-68% progression into HCC or other malignancy by 24 months [49-51]. The AASLD surveillance and diagnostic algorithm also links LI-RADS categories with management recommendations.
CEUS was previously recommended in the 2005 AASLD guidelines as part of the diagnostic algorithm [52]. However, CEUS were not recommended in the 2011 or 2018 versions and not included in the AASLD diagnostic algorithm, unlike the four other guidelines which either include CEUS as a first-line or second-line imaging modality. The AASLD guidance document cites concerns mentioned in a meta-analysis [53], including: absence of a large-scale study, potential selection bias for patients with adequate quality ultrasounds, lack of generalizability of studies in Asia versus Western countries, and operator dependency.
Imaging criteria for arterial phase hyperenhancing HCC
LI-RADS category 5 is equivalent to the arterial phase hyperenhancing HCC. Defer to LI-RADS section below for the specific diagnostic criteria.
Imaging criteria for arterial phase iso- or hypoenhancing HCC
The guidelines do not permit the diagnosis of arterial phase isoor hypoenhancing HCC.
Imaging criteria for arterial phase iso- or hypoenhancing probable HCC
The guidelines allow arterial phase iso- or hypoenhancing observations to qualify as probable HCC (designated as LI-RADS 4) with different combinations of major imaging features. Defer to âdiagnostic scopeâ on LI-RADS section below for further details.
LI-RADS [10]
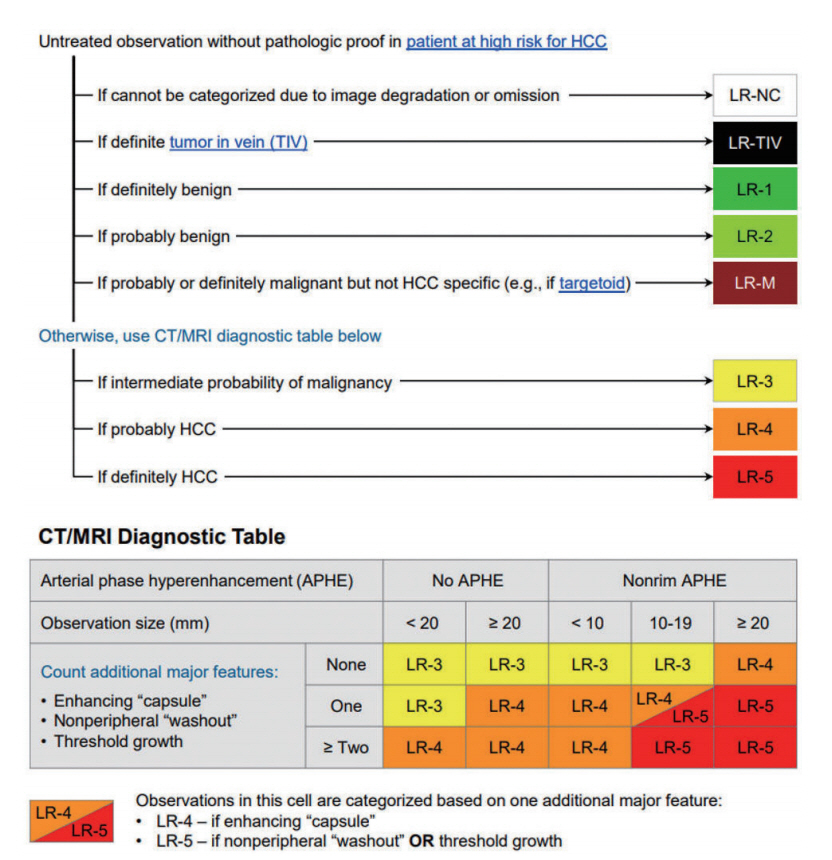
The CT/MRI diagnostic algorithm of HCC according to LI-RADS is presented in Figure 4.
Target population and tests for surveillance
The LI-RADS guidelines recommend ultrasound every 6 months for the surveillance of HCC in patients with liver cirrhosis of any etiology and non-cirrhotic HBV patients (Asian male >40 years old, Asian female >50 years old, African or North American Blacks with HBV, family history of HBV). The guidelines also defer to regional HCC clinical practice guidelines for additional indications in the absence of cirrhosis.
Target population and imaging modalities for diagnosis
The target population for the initiation of the diagnostic algorithm for HCC is broader compared to those for the surveillance; adult patients with cirrhosis of any cause except vascular disorder or congenital hepatic fibrosis, patients with chronic hepatitis B with or without cirrhosis, patients with current or prior HCC with or without cirrhosis, and adult liver transplantation candidates and liver transplant recipient.
First-line diagnostic imaging modalities includes not only dynamic CT or MRI with ECA or with HBA, but also CEUS. LI-RADS is the only guideline which permits the diagnosis of HCC with CEUS as the initial imaging modality. HCC can be diagnosed definitely on CEUS if observations equal or larger than 1 cm show APHE followed by late (>60 seconds) and mild washout (CEUS LR-5). Observations that show rim APHE, early (<60 seconds) washout or marked washout indicating probably or definitely malignant observations, but not HCC specific are assigned the CEUS LR-M category. Although CEUS has many advantages such as real-time imaging with high temporal resolution, safe and nonvisualization of vascular pseudolesions, LI-RADS CEUS also acknowledges its limitations: has fewer ancillary features, permits characterization of a limited number of targeted observations per examination (preferably those that are visible on precontrast US) and hence is not suitable for staging.
Imaging criteria for arterial phase hyperenhancing HCC
LI-RADS category 5 is equivalent to the arterial phase hyperenhancing HCC and the diagnostic criteria as follows:
Nodule size âĨ20 mm: -APHE and one or more of following: nonperipheral âwashoutâ, enhancing âcapsuleâ, or threshold growth.
Nodule size 10â19 mm: -APHE and nonperipheral washout or threshold growth.
-APHE and two or more of the following: nonperipheral washout, enhancing capsule, or threshold growth.
Imaging criteria for arterial phase iso- or hypoenhancing HCC
The guidelines do not permit the diagnosis of definite HCC (designated as LR-5) with arterial phase iso- or hypoenhancing observations.
Imaging criteria for arterial phase iso- or hypoenhancing probable HCC
The guidelines allow arterial phase iso- or hypoenhancing observations to qualify as probable HCC (designated as LR-4) with different combinations of major imaging features.
Diagnostic scope
LI-RADS is a comprehensive system designed to standardize the acquisition, interpretation and reporting of CT, MRI and CEUS examination of the liver in patients at risk for HCC and to provide precisely defined terminology, an illustrative atlas, a diagnostic algorithm, and guidance for appropriate imaging technique. Unlike other systems, LI-RADS addresses the full spectrum of lesions and pseudolesions encountered on imaging in patients at risk for HCC. Observations are classified into categories that reflect their relative probability benignity or malignancy (ranging from LR-1 to LR-5) or malignancy, not specific for HCC (LR-M) on the basis of CT, MRI, or CEUS findings [24,54].
LI-RADS also incorporates ancillary imaging features that modulate the likelihood of HCC. Radiologists may, at their discretion, apply ancillary features that favor HCC to upgrade the category by one or more categories (up to but not beyond LR-4) or apply ancillary features that may favor benignity to downgrade the category by one or more categories.
EASL
The diagnostic algorithm and recall policy in cirrhotic liver according to EASL is presented in Figure 5.
Target population and tests for surveillance
The EASL guidelines recommend ultrasound every 6 months for the surveillance of HCC in cirrhotic patients with Child-Pugh stage A/B or with stage C awaiting liver transplantation and in non-cirrhotic patients with HBV infection at intermediate or high risk for HCC or with F3 fibrosis regardless of etiology. Ultrasound less than 4-month interval is recommended when a sub centimeter nodule has been detected. CT or MRI may also be utilized for patients on waiting list for liver transplantation and for patients with inadequate ultrasound assessment is expected due to obesity, internal gas, and chest wall deformity.
Target population and imaging modalities for diagnosis
First-line diagnostic imaging modalities including MRI with HBA in addition to dynamic CT or MRI with ECA should be performed in patients at risk for HCC with âĨ1 cm nodule on surveillance ultrasound. EASL v 2018 newly permitted the use of CEUS as a secondary imaging modality for the diagnosis of hypervascular HCC.
Imaging criteria for arterial phase hyperenhancing HCC
For observations larger than 1 cm, the combination of APHE and washout appearance is required for the diagnosis of arterial phase hyperenhancing HCC. Contrary to the KLCA-NCC guidelines v 2018, the EASL guidelines only allow a narrow definition of âwashoutâ as hypointensity only on the portal venous phase in HBA-enhanced MRI.
Imaging criteria for arterial phase iso- or hypoenhancing HCC
The guidelines do not permit the diagnosis of arterial phase isoor hypoenhancing HCC.
Imaging criteria for arterial phase iso- or hypoenhancing probable HCC
The guidelines do not permit the diagnosis of arterial phase isoor hypoenhancing probable HCC.
Diagnostic scope
Among the five guidelines discussed in this review article, EASL provides the narrowest diagnostic scope for HCC by using the following diagnostic criteria for nodules âĨ1 cm: arterial phase hyperenhancement and washout on the portal venous phase or delayed phase on CT and MRI studies using ECA or washout on the portal venous phase on HBA-enhanced MRI. The guidelines do not approve the diagnosis of HCC or probable HCC for nodules with isoor hypovascularity and does not apply any ancillary features that may modulate the likelihood of HCC.
LIMITATIONS AND FUTURE DIRECTIONS
There are some limitations of the current systems that need to be addressed.
First, the systems vary reflecting differences in technology, cultural factors, clinical practice patterns, and management strategies. Although these differences among the systems may be unavoidable, radiologists must adapt to the difference between these systems. The current absence of unification and standardization of HCC imaging systems poses many disadvantages such as limitation on the development of registries, sharing of data and adoption of scientific advances developed from other systems; classification of the same nodule differently depending on the diagnostic systems; and hindrance of knowledge dissemination from other institutions adopting different systems. The unification and standardization of HCC imaging systems may be anticipated after the identification of potential barriers and the harmonization of different aspects of diverse systems.
Second, a definite diagnosis of HCC is not allowed for small (<1 cm) nodules or arterial iso- or hypoenhancing HCCs in most guidelines except APASL. Indeed, rendering a reliable diagnosis for small nodules (<1 cm) on CT or MRI as HCC may be difficult due to the low probability of HCC [22,38]. Also, for the sake of high specificity in the diagnosis of HCC, encompassing atypical and hypovascular lesions for the diagnosis of HCC may pose challenges. However, considering the high progression rate (approximately more than 90%) of subcentimeter hypervascular nodules with typical HCC imaging findings on gadoxetic acid enhanced MRI to typical HCCs [55,56] and improved prognosis of very early stage HCCs compared to early-stage HCCs [38,57], the diagnosis of subcentimeter HCCs can be of clinical benefit. Furthermore, instead of excluding the diagnosis of HCC to all nodules with arterial iso- or hypoenhancing nodules on CT or MRI, additional investigation using other imaging modalities may be warranted to avoid missing HCCs. This is best illustrated by APASL which recommends using CEUS with SonazoidÂŪ to characterize hypovascular nodules on initial CT or MRI.
Third, although there has been a trend toward the use of CEUS as a secondary modality, as endorsed by EASL, KLCA-NCC, and APASL, there is scarce evidence justifying the selection of the most appropriate second-line imaging modality after an initial inconclusive examination and comparative evidence between different CEUS contrast agents. Only APASL accepts the use of Sonazoid ÂŪ whereas most other guidelines including EASL, LI-RADS, and KLCA-NCC accept the use of pure blood-pool contrast agents such as SonoVueÂŪ. Therefore, further prospective studies involving a larger number of patients are warranted to confirm the role of CEUS as the most effective secondary modality and head-tohead studies are required to compare the diagnostic performance between CEUS agents.
Lastly, additional imaging methods other than dynamic imaging, such as diffusion-weighted imaging or HBP can be included in the diagnostic criteria to compensate the imperfect sensitivity and specificity of the current noninvasive diagnostic criteria. There is a trend for the adoption of these additional imaging methods. For example, LI-RADS and KLCA-NCC guidelines include restricted diffusion as an ancillary feature favoring malignancy in general, and marked T2 hyperintensity as an ancillary feature favoring benignity. Furthermore, HBA-enhanced MRI may further be utilized widely considering the potential benefit of the characterization of lesions on the basis of both vascularity and hepatocellular uptake [58].
CONCLUSION
Several scientific organizations have proposed systems that incorporate imaging for surveillance and diagnosis for HCC. The designs and component of these systems differ considerably reflecting different target populations, resources, and treatment practices. In 2018 particular, LI-RADS, AASLD, EASL, and KLCANCC have been updated. Key changes include wider recognition of hepatobiliary agents and CEUS, expecting the increased role in both modalities in the noninvasive diagnosis of HCC in the years to come. Integration of LI-RADS into the AASLD practice guidance also announces future harmonization and unification of diagnostic imaging systems to facilitate knowledge dissemination. Yet, several issues remain to be solved regarding the diversity of the systems, diagnosis of subcentimeter HCCs and hypovascular HCCs, evaluation of CEUS as an appropriate second-line modality, the head-to-head comparaison of different CEUS contrast agents (SonoVueÂŪ and SonazoidÂŪ), and adoption of ancillary imaging features seen not assessed on dynamic imaging. In the near future, these issues can be clarified on the basis of large-scale data-driven evidence.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print





