Efficacy and safety of ledipasvir/sofosbuvir in 5,028 Mongolian patients infected with genotype 1 hepatitis C virus: A multicenter study
Article information
 , Sang Hoon Ahn,2, Nyamsuren Naranzul1,4, Damba Enkhtuya4,5, Nagir Choijamts4,5, Purev Batbayar4,5, Radnaa Otgonbayar6, Bat-Ulzii Saruul4,7, Chuluunbaatar Gantuul4,7, Baljinnyam Gegeebadrakh4,8, Narangerel Tuvshinbayar4,8, Dorjgotov Badamsuren4,9, Galsan Ulzmaa4,9, Jamiyandorj Otgonbold10, Kwang-Hyub Han2
, Sang Hoon Ahn,2, Nyamsuren Naranzul1,4, Damba Enkhtuya4,5, Nagir Choijamts4,5, Purev Batbayar4,5, Radnaa Otgonbayar6, Bat-Ulzii Saruul4,7, Chuluunbaatar Gantuul4,7, Baljinnyam Gegeebadrakh4,8, Narangerel Tuvshinbayar4,8, Dorjgotov Badamsuren4,9, Galsan Ulzmaa4,9, Jamiyandorj Otgonbold10, Kwang-Hyub Han2
Abstract
Background/Aims
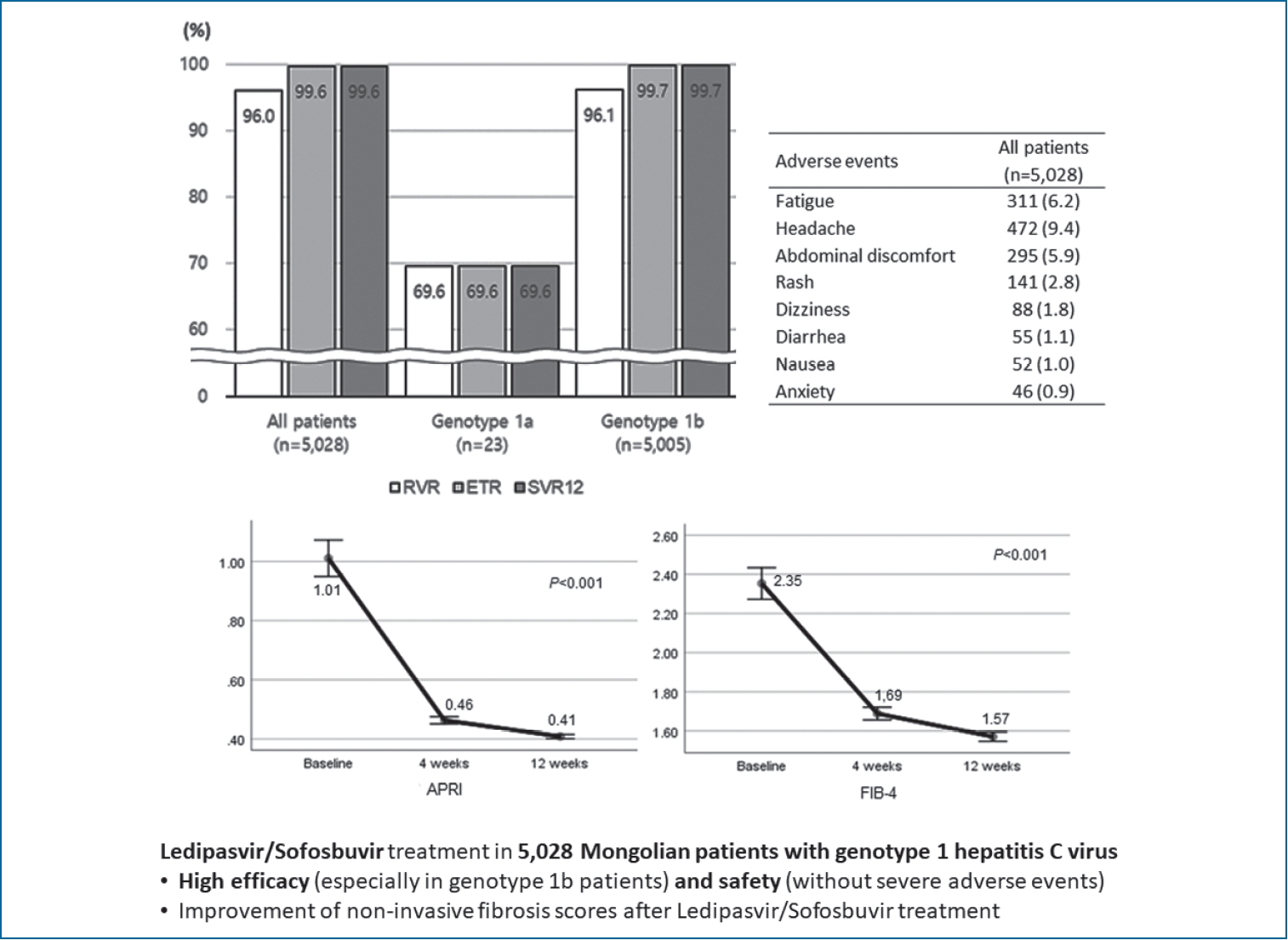
Ledipasvir/sofosbuvir (LDV/SOF) shows high efficacy and safety in patients with genotype 1-hepatitis C virus (HCV). We aimed to investigate the efficacy and safety of LDV/SOF in real-world Mongolian patients.
Methods
Between 2015 to 2019, 23 (0.5%) and 5,005 patients (99.5%) with genotype 1a and 1b HCV, respectively, were treated with a fixed-dose tablet containing 90 mg ledipasvir and 400 mg sofosbuvir for 12 weeks, and 81 patients (1.6%) with previous experience of interferon (IFN)-based treatment received additional 1,000 mg ribavirin. HCV RNA was measured at 4, 12, and 24 weeks after the first dose to determine rapid virologic response, end of treatment response (ETR), and sustained virologic response at 12 weeks after end of treatment (SVR12).
Results
Most patients (n=5,008; 99.6%) achieved ETR and SVR12 without virologic relapse. Patients with genotype 1a showed low rates of ETR and SVR12 in only 16 patients (69.6%). There was no significant difference in SVR12 rate between patients regardless of IFN experience (n=81; 1.6%), cirrhosis (n=1,151; 22.9%), HCV RNA >6×106 IU/mL (n=866; 17.2%), or liver stiffness >9.6 kPa (n=1,721; 34.2%) (100.0%, 99.3%, 99.4%, and 99.4%, respectively). No severe adverse events (AEs) were reported, and there was no dose reduction or interruption due to AE. The most common AEs were headache (n=472; 9.4%), fatigue (n=306; 6.2%), abdominal discomfort (n=295; 5.9%), and skin rash (n=141; 2.8%).
Conclusions
LDV/SOF showed high efficacy and safety for patients with genotype 1, especially 1b HCV, in Mongolia. The real-world data might be applicable to patients in other Asian-Pacific countries.
Graphical Abstract
INTRODUCTION
The prevalence of hepatitis C virus (HCV) infection in Mongolia is estimated to be 15.6% based on a national seroepidemiologic data [1-3]. Such a high rate of HCV infection in Mongolia might be due to reuse of needles before 1990, traditional medicine including bloodletting, and other unsafe medical or dental procedures. Interestingly, the most common HCV genotype in Mongolia was found to be 1b, accounting for 98% of all genotypes [2].
Since the introduction of direct-acting antivirals (DAAs) including boceprevir and telaprevir in 2011, the new DAA ledipasvir/sofosbuvir (LDV/SOF) in 2014 opened a new era of interferon-free, all-oral agents for HCV treatment [4]. A fixed dose of ledipasvir, a NS5A inhibitor, and sofosbuvir, a nucleotide analogue NS5B polymerase inhibitor, showed a promising antiviral efficacy and safety in genotype 1 HCV-infected patients. In a phase 3 pivotal study, the overall sustained virologic response (SVR) rates were 99% in treatment-naïve patients who received 12 weeks of LDV/SOF [5]. Moreover, in genotype 1 HCV patients who had experienced prior interferon-based treatment, 12 weeks of LDV/SOF plus ribavirin resulted in 96% of SVR rates [6].
In the era of interferon or pegylated interferon (PEG-IFN), Mongolian patients rarely underwent antiviral therapy because the cost was high and the access to medical resources was significantly limited. However, according to the approval of the implementation of the Hepatitis Prevention, Control and Elimination Program between 2016 and 2020 by the Mongolian government, treatment campaign for HCV started from January 2016. Fortunately, Gilead Sciences, Inc. has successfully implemented an access program, in which the cost of LDV/SOF was remarkably reduced to 300 US dollars per bottle. To date, more than 10,000 Mongolian patients infected with HCV have received brand LDV/SOF (Harvoni®; Gilead Sciences, Inc., Foster City, CA, USA).
There have been few real-life data regarding brand or generic LDV/SOF for HCV patients worldwide [7]. However, the sample size was small. Thus, the aim of this study was to report the efficacy and safety of brand LDV/SOF in 5,028 Mongolian patients infected with genotype 1 HCV who received LDV/SOF or LDV/SOF plus ribavirin for 12 weeks.
PATIENTS AND METHODS
Patients eligibility
In this retrospective cohort study, patients who met the following criteria were included: 1) patients aged 18–70 years; 2) patients with chronic HCV infection documented by anti-HCV or by patient’s statement; 3) patients with HCV genotype 1a or 1b; 4) treatment-experienced or -naïve patients; 5) patients with negative results for hepatitis A and B as well as human immunodeficiency virus (HIV); 6) patients without decompensation of liver function, such as ascites and hepatic encephalopathy; 7) patients without diagnosis of hepatocellular carcinoma at enrollment; 8) patients with normal value of baseline serum alpha-fetoprotein; 9) patients with normal range of baseline serum creatinine; 10) patients who have completed follow-up for 12 weeks after the end of treatment (EOT); and 11) patients who were treated with only brand LDV/SOF.
Laboratory tests and data collection
All included patients were subjected to laboratory tests at the beginning of treatment, including complete blood count (CBC), alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin, serum albumin, prothrombin time, IgG anti-hepatitis A virus, hepatitis B virus surface antigen, anti-HIV, and antiHCV. Anti-HCV reactivity was assayed using a HISCL 5000 analyzer (Sysmex Corp., Kobe, Japan), and serum HCV RNA was quantitated using a Roche COBAS® TagMan HCV Test (V3.0, cutoff value, 15 IU/mL; Roche Molecular Systems, Branchburg, NJ, USA). HCV genotyping was performed using a gene sequencing assay.
Laboratory tests, including CBC, ALT, AST, total bilirubin, serum albumin, prothrombin time, and serum HCV RNA quantitation, were repeated at 4 weeks, EOT, and 12 weeks after EOT.
Ultrasonographic evaluation and liver stiffness measurement
Before administration of LDV/SOF, baseline ultrasonographic examination and liver stiffness measurement (LSM) using transient elastography (FibroScan®, Echosens, Paris, France) were conducted. LSM was performed by a single experienced technician who was blinded to the patient information. The results were expressed as kilopascals (kPa), and the interquartile range (IQR) was defined as an index of intrinsic variability of LSM corresponding to the interval of LSM results containing 50% of the valid measurements between the 25th and 75th percentiles. The median value was considered representative of the elastic modulus of the liver. Only procedures with at least 10 valid measurements, a success rate of at least 60%, and an IQR to median value ratio of 30% were considered reliable [8-10]. The cutoff value was considered as 8.4 kPa for F2, 9.6 kPa for F3, and 12.8 kPa for F4 fibrosis according to a recent study [11]. Because patients were subjected to LSM at baseline with active inflammation, overassessment of LSM could occur. Therefore, in this study, nodular liver surface combined with blunted edge in ultrasonographic evaluation and high liver stiffness (LS) value (>12.5 kPa) was considered as a relative definition of liver cirrhosis [12].
Because repeated transient elastography was not feasible in Mongolia, AST to platelet ratio index (APRI; APRI = AST / 41 [as the upper limit of normal AST] / platelet count) and fibrosis-4 (FIB-4) index (FIB-4 index = age × AST / [platelet count × ALT1/2]), which are simple non-invasive fibrosis scoring systems, were calculated at each time point during treatment. Cutoff of significant and severe fibrosis were considered as 0.7 and 1.0 in APRI, and 1.45 and 3.25 in FIB-4, respectively [11,13].
Antiviral therapy
Patients with genotype 1a or 1b received a fixed-dose combination tablet containing 90 mg ledipasvir and 400 mg sofosbuvir for 12 weeks, as only 12-week regimen was approved in Mongolia. If patients had a prior experience of PEG-IFN treatment for HCV, they received an additional fixed dose of 1,000 mg ribavirin during LDV/SOF treatment [5,6,14].
Assessment of antiviral efficacy and safety
The primary efficacy endpoint was SVR, defined as undetectable HCV RNA at 12 weeks after EOT (SVR12). Rapid virologic response (RVR) and EOT response (ETR) were defined as completely undetectable HCV RNA at 4 weeks and EOT, respectively. The virologic relapse was defined as a detectable HCV RNA level after EOT in a patient who had undetectable HCV RNA during treatment. Non-response was defined as a detectable HCV RNA at EOT in a patient who did not experience virologic breakthrough. Any adverse events (AEs) that developed during antiviral therapy were recorded.
Statistical analysis
Continuous variables were expressed as median and IQR. Categorical variables were presented by frequency and percentage. Differences between continuous and categorical variables were examined for statistical significance using Student’s t-test (or the Mann-Whitney test, as appropriate) and the chi-squared test (or Fisher’s exact test, as appropriate). A generalized linear model using repeated measured analysis of variance (ANOVA) was used to assess the longitudinal changes in variables with a Bonferroni correction for multiple comparisons. Multivariate analysis was performed with adjustments for significant variables with P<0.05 in the univariate analyses using logistic regression model. Continuous variables were categorized using cutoffs that were clinically used or obtained with reference to the receiver operating characteristic (ROC) curve, and entered into the univariate and multivariate analyses. The odds ratio (OR) for SVR12 and its 95% confidence interval (CI) were calculated for each selected variable. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS version 25.0; IBM, Armonk, NY, USA). A P value <0.05 was considered statistically significant.
RESULTS
Baseline characteristics and on-treatment laboratory tests
According to the Hepatitis Prevention, Control and Elimination Program of the Mongolian government from January 2016, there were more than 10,000 patients treated with brand LDV/SOF for genotype 1 HCV between December 2015 and June 2019, and 5,449 patients completed follow-up for 12 weeks after the EOT. After excluding 421 patients, 5,028 patients who met the inclusion criteria were retrospectively analyzed (Fig. 1).

Flowchart of patient enrollment. HCV, hepatitis C virus; LDV/SOF, ledipasvir/sofosbuvir.
Baseline characteristics and on-treatment laboratory tests of the 5,028 patients are described in Table 1 and Supplementary Table 1. The median age was 54.0 years (IQR, 45.0–62.0). The proportion of male patients was 46.2% (n=2,324). Liver cirrhosis was clinically diagnosed in 1,151 patients (22.9%). Additional ribavirin was administered during LDV/SOF treatment in only 81 (1.6%) genotype 1b patients who had previous PEG-IFN experience. The median AST and ALT levels were slightly high (50.5 and 63.8 IU/L) at baseline. The median baseline LS value was 8.0 kPa (IQR, 5.4–11.7), and 1,721 patients (34.2%) showed LS value >9.6 kPa.

Baseline characteristics and laboratory tests according to hepatitis C virus subtype and previous interferon-based therapy
Almost all (n=5,005; 99.5%) patients had HCV genotype 1b. Between genotype 1a and 1b, there was no significant difference at baseline regardless of sex distribution (69.6% vs. 46.1% of male sex, P=0.027), body mass index (median 29.1 vs. 28.2 kg/m2, P=0.019), and FIB-4 index (median 2.58 vs. 1.76, P=0.037). At 4 weeks, genotype 1a patients showed slightly low serum albumin level (median 4.0 vs. 4.2 g/dL) as well as high prevalence of APRI above 1.0 (21.7% vs. 5.8%) and FIB-4 above 3.25 (21.7% vs. 6.9%) (all P<0.05).
PEG-IFN-experienced patients tended to have higher baseline HCV RNA (log value 6.06 vs. 5.68, P=0.002). However, other variables were not significantly different between patients with or without PEG-IFN experience.
Treatment outcomes
Of total 5,028 patients with HCV genotype 1 infection, 5,008 (99.6%) had successful HCV disappearance after 12 weeks of antiviral therapy. RVR, ETR, and SVR12 were analyzed in 4,825 (96.0%), 5,008 (99.6%), and 5,008 patients (99.6%). All patients who showed RVR achieved ETR later, and patients who achieved ETR finally reached SVR12 without virologic relapse. RVR, ETR, and SVR12 were achieved by 69.6% (n=16), 69.6%, and 69.6% of 23 patients with genotype 1a, respectively. In contrast, the rates of RVR, ETR, and SVR12 in 5,005 patients with genotype 1b were 96.1% (n=4,809), 99.7% (n=4,992), and 99.7%, respectively. Most patients showed ETR and RVR regardless of the presence of PEG-IFN experience, high baseline HCV RNA (>6×106 IU/mL), liver cirrhosis or indicators of advanced fibrosis including high LS, APRI, and FIB-4 values (Fig. 2, Supplementary Table 2).
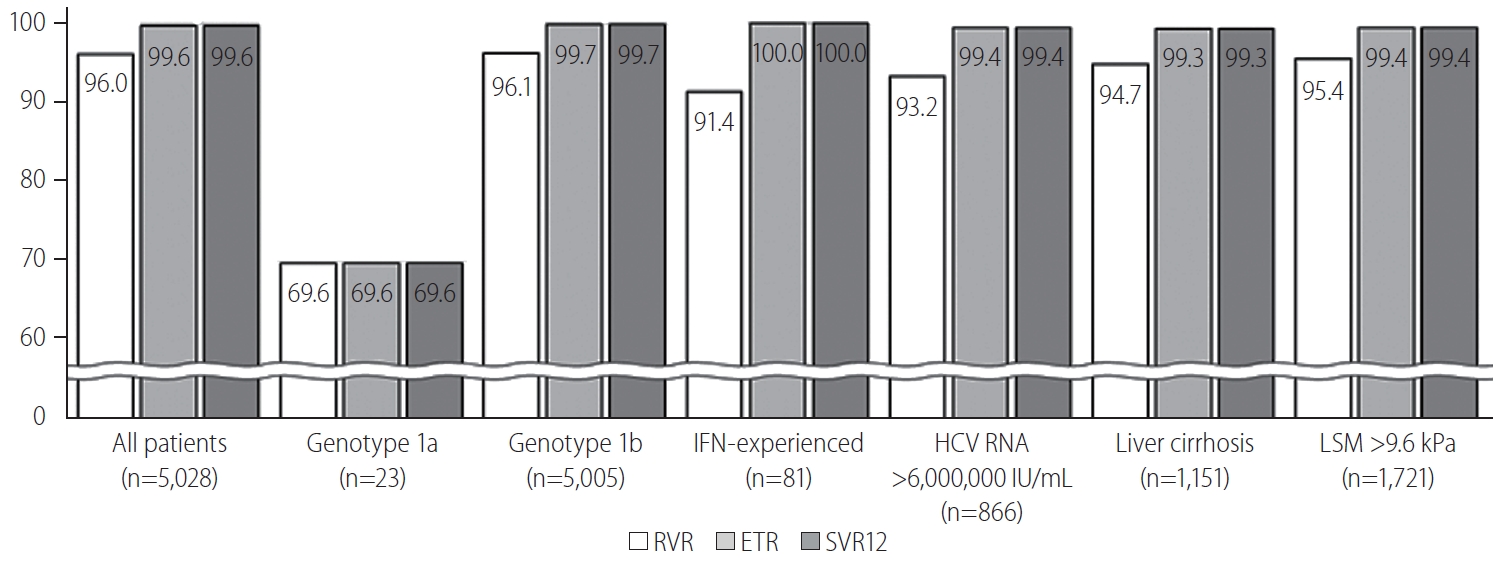
Rates of RVR, ETR, and SVR12. IFN, interferon; HCV, hepatitis C virus; LSM, liver stiffness measurement; RVR, rapid virological response; ETR, early virological response; SVR12, ustained virological response after 12 weeks of treatment.
Laboratory result changes during antiviral therapy
Changes in the estimated marginal mean of laboratory test results during antiviral therapy are described in Figure 3 and Supplementary Table 3. The estimated mean values of baseline AST and ALT levels were 68.9±0.7 and 85.0±0.3 IU/L, significantly decreased to 32.3±0.3 and 36.5±0.4 IU/L at 4 weeks, and further decreased to 29.2±0.2 and 32.7±0.2 IU/L at EOT, respectively (all P<0.001). The estimated mean value of total bilirubin also decreased (0.96 to 0.78 mg/dL, P<0.001), and the mean serum albumin was slightly elevated (4.2 to 4.3 g/dL, P<0.001) during antiviral therapy. Platelet count tended to slightly decrease, but almost similar (200.8/mm3 to 196.8/mm3, P<0.001). The estimated mean values of APRI and FIB-4 also reliably decreased (1.01 to 0.41 and 2.35 to 1.57, respectively; all P<0.001).
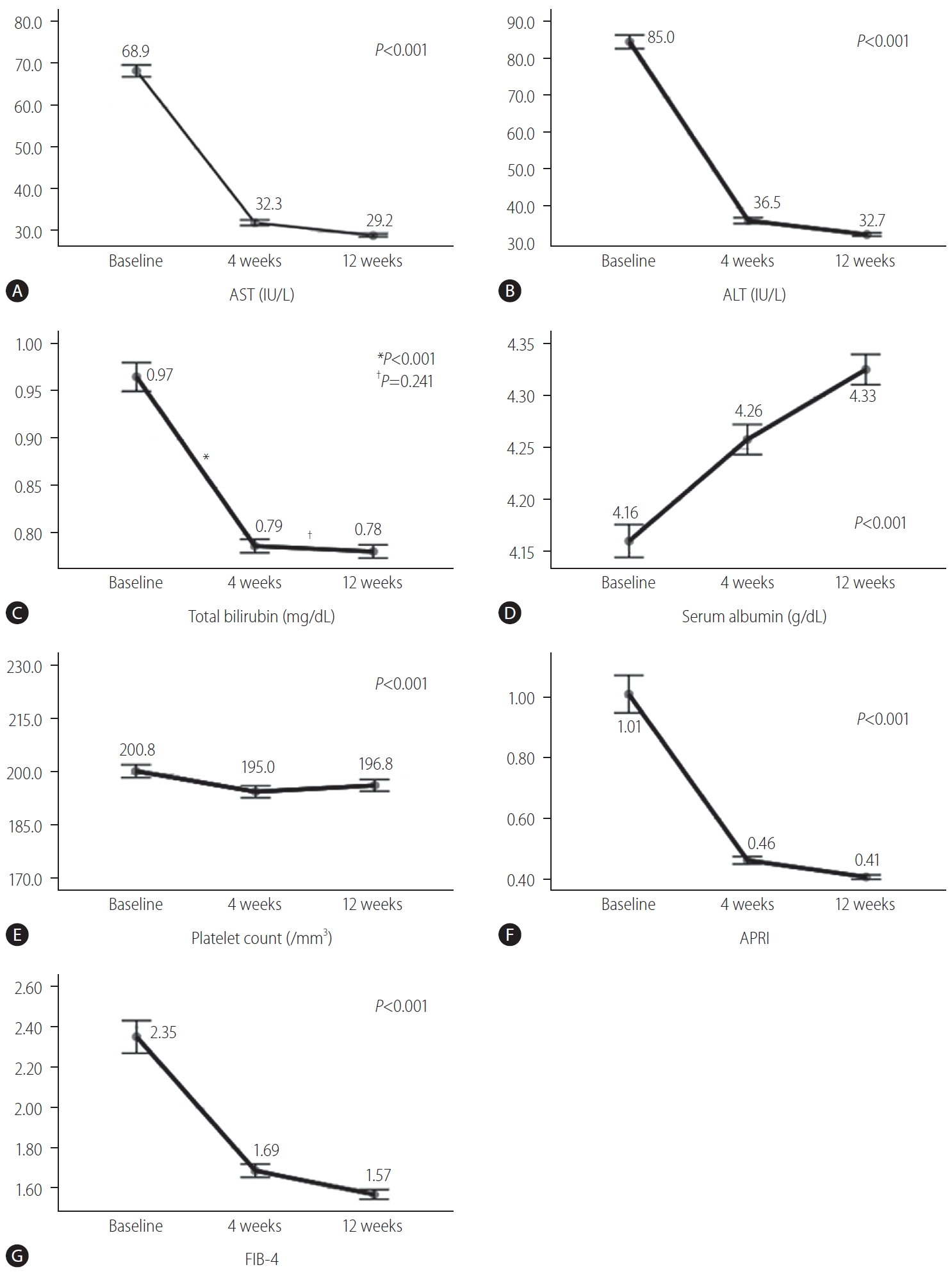
Estimated marginal mean changes in laboratory test results and non-invasive fibrosis index after ledipasvir/sofosbuvir treatment: (A) aspartate aminotransferase (AST), (B) alanine aminotransferase (ALT), (C) total bilirubin, (D) serum albumin, (E) platelet count, (F) AST to platelet ratio index (APRI), and (G) fibrosis-4 index (FIB-4). *P<0.001. †P=0.241.
Virologic breakthrough after non-response
Estimated mean HCV RNA quantitation in 20 patients (0.4%) who showed non-response decreased until the EOT (5.97±0.28 to 3.39±0.08 log IU/mL, P<0.001). However, at 12 weeks after the EOT, the log value of HCV RNA in non-responders was elevated to 4.79±0.14 (P<0.001), which corresponded to virologic relapse after incomplete virologic response (Fig. 4, Supplementary Table 4).
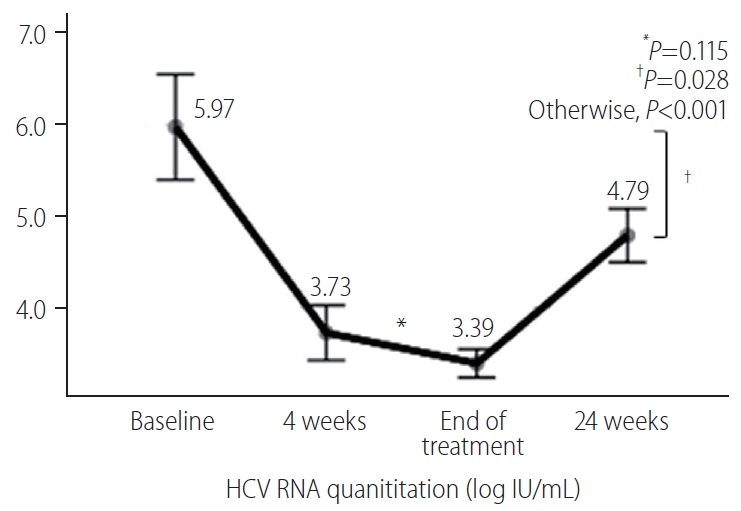
Estimated mean changes in log value of HCV RNA after treatment in 20 patients who failed to achieve end-treatment response and sustained virologic response. HCV, hepatitis C virus. *P=0.115. †P=0.028.
Variables associated to ETR and SVR12
In univariate analysis, variables at baseline, such as the presence of liver cirrhosis, high HCV RNA (>1.12×106 IU/mL, cutoff by ROC curve), high LS (>9.6 kPa), and high FIB-4 (>3.25), and variables at 4 weeks, such as high bilirubin, low albumin, low platelet count, and APRI and FIB-4 above each cutoff, showed significant association with ETR and SVR12 achievement (all P<0.05) (Supplementary Table 5). Multivariate analyses at each time point based on these variables were subsequently performed (Table 2). At baseline, high FIB-4 (>3.25) (OR, 0.356; P=0.025) showed reversed association with ETR and SVR12 achievement. At 4 weeks of treatment, non-invasive fibrosis scoring, such as APRI >0.7 (OR, 0.248), APRI >1.0 (OR, 0.283), and FIB-4 >3.25 (OR, 0.263) showed reversed association with ETR and SVR12 achievement, with serum albumin below 3.5 g/dL (all P<0.05).
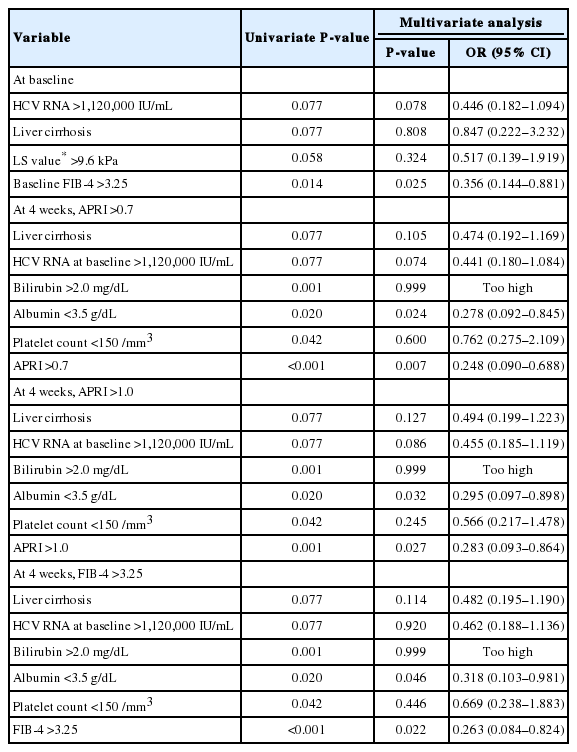
Multivariate analysis for complete end-treatment response and sustained virologic response at 12 weeks after treatment
AEs during antiviral therapy
During 12 weeks of antiviral therapy, the most common AEs were headache, fatigue, abdominal discomfort, and skin rash, which occurred in 472 (9.4%), 311 (6.2%), 295 (5.9%), and 141 patients (2.8%). There was no difference in AE development between IFN-experienced and -naïve groups (Table 3).
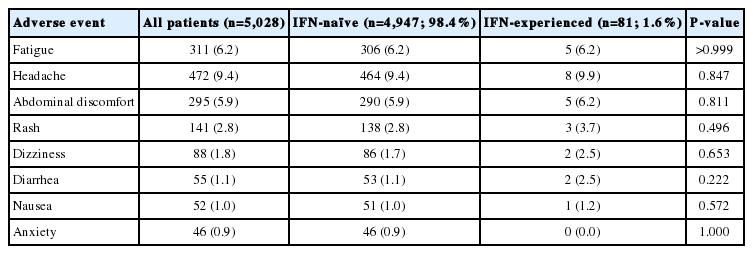
Adverse events during antiviral therapy
DISCUSSION
In this real-world cohort study, 12-week treatment with LDV/SOF (±ribavirin) showed high effectiveness in 5,028 Mongolian patients infected with genotype 1 HCV, regardless of previous IFN experience. Compared with that in patients with genotype 1b (99.6%), SVR rate in genotype 1a was very low (69.6%) compared with that in previous studies; however, the number is relatively small (n=23; 0.5%). Non-responders (n=20; 0.4%) also experienced reduction of viral load through 12 weeks of treatment with LDV/SOF; however, after the EOT, subsequent virologic breakthrough occurred in the 20 patients. No serious AE occurred during LDV/SOF treatment.
Similar to western guidelines, the recent Asian-Pacific guideline is based on the new era of DAAs on HCV treatment [15,16]. Many DAAs are currently in use, and currently, pangenotypic DAAs such as sofosbuvir/velpatasvir and glecaprevir/pibrentasvir tend to be increasingly preferred. However, pangenotypic DAAs are not always affordable in some developing Asian-Pacific countries owing to relatively low healthcare budgets and resources. Nevertheless, LDV/SOF is a well-known powerful DAA for genotype 1 HCV that showed 93% to 100% SVR rate. Recent European and Asian-Pacific guidelines still recommend 8–12 weeks of LDV/SOF for genotype 1b and treatment-naïve genotype 1a, 4, 5, and 6 [15,16]. As this study was conducted in conjunction with a drug-producing company as part of a Mongolian healthcare program from 2016, approvement of the regimen was restricted to 12 weeks of LDV/SOF and ribavirin addition for treatment-experienced patients in Mongolia [5,6,17,18].
To the best of our knowledge, this is the largest real-life study for genotype 1 HCV treated with LDV/SOF in a single country. The distribution of HCV genotypes was shown to be quite homogeneous in Mongolia in a previous study, which revealed that genotype 1b accounted for 98.8% of all genotypes in Mongolia [1]. In this study, which was limited to genotype 1 HCV, 99.5% of patients had genotype 1b HCV. Such a high proportion of genotype 1b in Mongolian patients might be appropriate for LDV/SOF treatment, which showed an even higher overall SVR rate of 99.6% in genotype 1 than that in previous clinical trials [15,16].
No virologic relapse was observed until 12 weeks after the EOT in this study. However, subsequent elevation of viral load was shown to be occur in 20 treatment-failure cases. A recent Japanese study suggested factors such as cirrhosis (OR, 4.19; P=0.014) and resistance-associated substitutions (RASs) in NS5A at baseline (OR, 7.78; P<0.001), and other phase II and III trials also showed relatively low SVR12 with NS5A RAS (91% compared with 99% without NS5A RAS) [19,20]. In this study, accurate diagnosis of cirrhosis using tissue biopsy or sequential LSM was limited, and analysis for NS5A RAS was not available. Instead, we used non-invasive fibrosis indices, such as APRI and FIB-4, which showed significant association with EOT and SVR12 in multivariate analysis. This result may be considered to be related to the maintenance of treatment for a relatively long period of time in patients with cirrhosis or patients who have failed treatment in the existing guidelines, and might be interpreted as using baseline or on-treatment non-invasive fibrosis markers that also can predict the failure of LDV/SOF treatment. In addition, the viral load of patients who failed to achieve ETR and SVR decreased during treatment, but increased again after treatment. This may be interpreted as that additional doses or another DAAs should be considered for patients with poor response after 12 weeks of treatment.
Serious AE associated with LDV/SOF was not observed. The AE profiles in this study were not different from those in previous clinical trials. The most frequent AE was headache followed by fatigue, and there was no AE that resulted in dose interruption or treatment discontinuation. Consequently, LDV/SOF or LDV/SOF+ ribavirin may be safe for genotype 1 HCV-infected patients in real practice.
However, there are several limitations in this study. Firstly, LDV/SOF is not a novel DAA treatment and is already substituted with pangenotypic DAAs. Although LDV/SOF treatment is not a novel issue, this large-scale cohort study was aimed to show the efficacy and safety of an affordable DAA for developing countries such as Mongolia. This study could be a good example of successful hepatitis C treatment practice in developing countries where healthcare budgets are limited. Secondly, serum markers indicating tumor markers and renal functions were not analyzed. Thirdly, long-term SVR and its effect were not analyzed.
In conclusion, our data showed that LDV/SOF (±ribavirin) regimen for 12 weeks was highly effective and safe for genotype 1 HCV-infected patients in the real-world setting, especially in patients with genotype 1b. Such results might be translated into other patients infected with HCV genotype 1 living in other Asian-Pacific area as a part of worldwide HCV eradication.
Notes
Authors’ contribution
O Baatarkhuu, JS Lee and J Amarsanaa: study concept and design, data acquisition, analysis, and interpretation; statistical analysis and manuscript drafting. DY Kim and SH Ahn: study concept and design, data analysis, and interpretation; manuscript drafting and critical revision; and study supervision. N Naranzul, D Enkhtuya, N Choijamts, P Batbayar, R Otgonbayar, BU Saruul, C Gantuul, B Gegeebadrakh, N Tuvshinbayar, D Badamsuren, G Ulzmaa, J Otgonbold and KH Han: data acquisition and critical manuscript revision.
Conflicts of Interest: The authors have no conflicts of interests to disclose.
Acknowledgements
We greatly appreciate the cooperation of the Ministry of Health of Mongolia, University General Hospital of the Mongolian National University of Medical Sciences, Mongolian Academy of Medical Sciences, Happy Veritas Liver Diagnostics Center, National Center for Communicable Diseases, Second State Central Hospital, Third State Central Hospital and the Mongolian Association for the Study of Liver Diseases for their provision of field staff.
We would like to express our special appreciation to Yonsei University College of Medicine of Korea for their tremendous efforts in the presenting study.
SUPPLEMENTAL MATERIAL
Supplementary material is available at Clinical and Molecular Hepatology website (http://www.e-cmh.org).
Laboratory test results after treatment according to hepatitis C virus subtype and previous interferon-based therapy
Rates of complete treatment response at 4 weeks, end of treatment, and 12 weeks after treatment
Estimated mean change in laboratory test results after treatment
Estimated mean change in log value of HCV RNA after treatment in patients who did not achieve end-treatment response and sustained virologic response
Univariate logistic regression analysis for complete end-treatment response and sustained virologic response at 12 weeks after treatment
Abbreviations
AEs
adverse events
ALT
alanine aminotransferase
APRI
aspartate aminotransferase to platelet ratio index
AST
aspartate aminotransferase
CBC
complete blood count
CI
confidence interval
DAAs
direct-acting antivirals
EOT
end of treatment
ETR
end of treatment response
FIB-4
fibrosis-4
HCV
hepatitis C virus
HIV
human immunodeficiency virus
IQR
interquartile range
LDV/SOF
ledipasvir/sofosbuvir
LS
liver stiffness
LSM
liver stiffness measurement
OR
odds ratio
PEG-IFN
pegylated interferon
RASs
resistance-associated substitutions
ROC
receiver operating characteristic
RVR
rapid virologic response
SVR
sustained virologic response
References
Article information Continued
Notes
Study Highlights
We investigated the high efficacy and safety of ledipasvir/sofosbuvir regimen in real-world Mongolian patients with genotype 1 hepatitis C virus, especially in patients with genotype 1b. Although LDV/SOF treatment is not a novel issue, this large-scale cohort study was aimed to show the efficacy and safety of an affordable treatment for developing countries such as Mongolia. This study could be a good example of successful hepatitis C treatment practice in developing countries where healthcare budgets are limited.