Core indicators related to the elimination of hepatitis B and C virus infection in South Korea: A nationwide study
Article information

Abstract
Background/Aims
To eliminate hepatitis B virus (HBV) and hepatitis C virus (HCV) according to the World Health Organization (WHO) criteria in 2021, this study investigated the national core indicators representing the current status of viral hepatitis B and C in South Korea.
Methods
We analyzed the incidence, linkage-to-care, treatment, and mortality rates of HBV and HCV infection using the integrated nationwide big data of South Korea.
Results
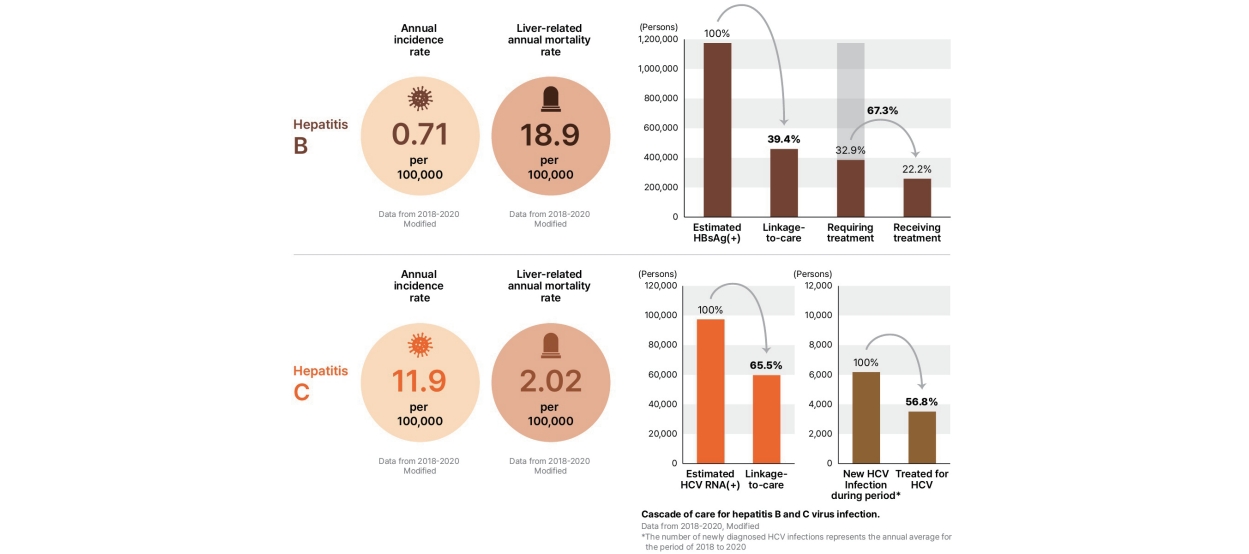
According to data from 2018–2020, the incidence of acute HBV infection in South Korea was 0.71 cases per 100,000 population; tthe linkage-to-care rate was only 39.4%. Among those who need hepatitis B treatment, the treatment rate was 67.3%, which was less than 80% reported in the WHO program index. The annual liver-related mortality due to HBV was 18.85 cases per 100,000 population, exceeding the WHO target of four; the most frequent cause of death was liver cancer (54.1%). The annual incidence of newly diagnosed HCV infection was 11.9 cases per 100,000 population, which was higher than the WHO impact target of five. Among HCV-infected patients, the linkage-to-care rate was 65.5% while the treatment rate was 56.8%, which were below the targets of 90% and 80%, respectively. The liver-related annual mortality rate due to HCV infection was 2.02 cases per 100,000 population.
Conclusions
Many of the current indicators identified in the Korean population did not satisfy the WHO criteria for validation of viral hepatitis elimination. Hence, a comprehensive national strategy should be urgently developed with continuous monitoring of the targets in South Korea.
Graphical Abstract
INTRODUCTION
The World Health Organization (WHO) estimated that 296 million people (3.8%) were living with chronic hepatitis B virus (HBV) infection worldwide, while 58 million people were living with hepatitis C virus (HCV) infection (0.75%) in 2019 [1]. Annually, about 1.3 million people die from viral hepatitis complications, including liver cirrhosis and hepatocellular carcinoma [2]. By 2040, the number of viral hepatitis-related deaths is expected to exceed the total number of deaths associated with HIV infection, tuberculosis, and malaria [3,4].
The WHO has declared viral hepatitis as a global public health problem, and urges various countries to implement measures to eliminate it. In 2016, the World Health Assembly adopted the Global Health Sector Strategy (GHSS) on viral hepatitis and set the goal of eliminating viral hepatitis by 2030 [5]. Emphasizing the joint efforts of the countries toward achieving the shared goal, the WHO published the interim guidance for country validation of viral hepatitis elimination, which sets impact targets and programmatic targets, in June 2021 [6]. The main impact indicators and targets for measuring elimination are as follows: 1) ≤0.1% HBV surface antigen (HBsAg) prevalence in those aged ≤5 years, 2) an absolute annual HCV incidence of ≤5 per 100,000 persons and of ≤2 per 100 persons who inject drugs (PWIDs), and 3) HBV- and HCVrelated annual mortality rates of ≤4 and ≤2 per 100,000 persons, respectively (combined HBV/HCV ≤6 per 100,000 persons).
In line with the WHO’s goal, various countries around the world, including the United States, Canada, United Kingdom, Taiwan, Japan, and Egypt, are implementing aggressive healthcare policies, including nationwide examination and treatment support, with some visible effects [7-12]. Recently, a series of country pilot studies based on the HBV/HCV elimination criteria were undertaken in seven countries, including Brazil, Egypt, Georgia, Mongolia, Rwanda, Thailand, and United Kingdom (England), and reports on the study results were distributed [13].
South Korea has introduced the national immunization of HBV and perinatal transmission prevention programs. The infant vaccination coverage reached 98%, while the HBsAg positivity among the age group 10–18 years was reduced to 0.1–0.2%. Also, the efficacy of the Korean health authorities’ elimination effort was validated for the first time in September 2008 in the Western Pacific region [14]. However, viral hepatitis remains a serious public health threat, as the HBsAg positivity rate is still 3–5% among adults aged ≥30 years [15], and no hepatitis C vaccine has been developed. Approximately 70% of liver cirrhosis cases and 80% of liver cancer cases in South Korea are due to HBV or HCV infection, which is a major cause of death in South Korea [16]. According to a recent disease-adjusted life year (DALY)-based analysis, HBV and HCV remain the leading causes of liver cancer DALYs and mortality in South Korea [17]. Therefore, it is crucial to establish national policies to reduce the incidence of viral hepatitis and liver related deaths in accordance with the new WHO elimination validation criteria. In this study, we aimed to estimate the national indicators (incidence, linkage-to-care, treatment, and liver-related mortality rates) for the development of viral HBV and HCV infection elimination strategies based on the 2021 WHO criteria.
MATERIALS AND METHODS
Source of data
This retrospective cohort study used the integrated nationwide big data of South Korea, including the Korea National Health and Nutrition Examination Survey (KNHANES) data from 2018 to 2020, the Infectious Disease Surveillance Data provided by the Korea Disease Control and Prevention Agency (KDCA) from 2018 to 2020, health insurance claims data provided by the Korean National Health Insurance Service (NHIS) from 2002 to 2020, and cause-of-death data from Statistics Korea (KOSTAT) from 2011 to 2020.
First, the KNHANES is a national surveillance system that has been assessing the health and nutritional status of Koreans since 1998. This nationally representative cross-sectional survey recruits 10,000 individuals each year as a survey sample. The KNHANES collects information on socioeconomic status, health-related behaviors, quality of life, healthcare utilization status, anthropometric measures, biochemical and clinical profiles of non-communicable diseases, and dietary intakes. Second, mandatory surveillance for acute HBV infection has been conducted by the KDCA since January 2016, while that for HCV infection was conducted since June 2017. Third, the NHIS database covers 97.1% of the Korean population and provides information on the vital status of the patients [18]. The data includes medical information (diagnosis, length of stay, treatment cost, and services received), prescription information (drug code, number of days prescribed, and daily dosage), income information, demographic information, and death date of the National Health Insurance subscribers [19]. Fourth, the cause-of-death data from Statistics Korea are classified based on the International Classification of Diseases 10th Revision (ICD-10) and the Korean Standard Classification of Diseases and Causes of Death. It contains information of almost the entire Korean population. Therefore, these databases have been previously validated as reliable resources for mortality research.
Study design
The incidence rate was calculated based on the infectious disease surveillance data provided by the KDCA, as well as the health insurance claims data provided by the NHIS of South Korea. The collection of infectious disease surveillance data for acute HBV infection started on January 7, 2016, according to the Case Definitions for National Notifiable Infectious Diseases, while that for newly diagnosed HCV infections, regardless of acute or chronic hepatitis C, as most of them were asymptomatic, started on June 3, 2017; accordingly, the surveillance data between 2018 and 2020 were used for determining the incidence rate of acute HBV infection and newly diagnosed HCV infection. The incidence rate was calculated using the infectious disease surveillance data and health insurance claims data from 2002 to 2020. Patients who were diagnosed with acute HBV infection or acute/chronic HCV infection within 3,650 days prior to the first report date (from 3,710 days to 60 days before the report date) were excluded.
In terms of linkage-to-care, the annual number of HBV or HCV infected patients was estimated using the KNHANES data from 2018 to 2020, with population weighting applied by year; meanwhile, the health insurance claims data from 2018 to 2020 were used to identify patients with HBV or HCV infection claims by year as patients in linkage-to-care.
Patients prescribed with antiviral drugs and assigned with HBV ICD-10 code in the health insurance claims data from 2018 to 2020 were presumed to receive antiviral treatment. The treatment rate of HCV infection was calculated using the number of patients who were prescribed with antiviral drugs out of those diagnosed with incident cases of HCV infection from 2018 to 2020.
For the analysis of deaths and causes of death, the number of patients with HBV or HCV infection was calculated based on the NHIS data obtained from 2011 to 2020. It was linked to the data from Statistics Korea to estimate the annual numbers. The summary of the operation definition is presented in Supplementary Table 1.
The NHIS approved the provided data following a review process, and the data were released with an encrypted number according to the disclosure principle. This study was approved by the institutional review board (CUH 2021-12-041). Informed consent was waived owing to the historical cohort nature of the study.
Definition of indices for HBV infection
The incidence of acute HBV infection was calculated using the infectious disease surveillance data from 2018 published by the KDCA; the data of those with two disease claims or more for the aforementioned disease within 3,650 days prior to the first report date (from 3,710 days to 60 days before report date) were excluded.
Among those with HBV infection, the linkage-to-care was calculated as the number of patients with two or more national health insurance claims divided by the estimated number of HBV infection patients. The estimated number of HBV was predicted based on the number of HBsAg-positive patients aged ≥10 years and calculated based on the KNHNES data (2018–2020). The HBV-infected patients within linkage-to-care referred to those aged ≥10 years, with two or more national health insurance claims for acute/chronic HBV infection as the main, sub, or third diagnosis code between 2018 and 2020. The hepatitis B diagnostic ICD-10 code used include B16 (B16, B16.0, B16.2, and B16.9), B17.0, B18.0, and B18.1.
The treatment rate was defined as the number of persons with chronic HBV infection who are currently receiving treatment of the estimated population living with chronic hepatitis B eligible for treatment. Numerator was calculated as the number of HBV-infected patients prescribed with antiviral drugs. Patients aged ≥10 years who were prescribed with antiviral drugs at least once for HBV infection as the main, sub, or third diagnosis code according to the 2018–2020 NHIS claims data were presumed to receive antiviral treatment. Denominator was calculated as the estimated number of HBV patients that required treatment, which was estimated according to the current standard of treatment, at the presumed proportion of patients requiring treatment—25% for chronic HBV infection, 88% for liver cirrhosis, and 100% for liver cancer—in reference to the previous studies [20].
HBV-related mortality was defined as the number of liver-related deaths caused by K70–76 and C22 among people with HBV infection that occurred in the year/standard population of the year. The HBV-infected patients were identified by counting those who had two or more national health insurance claims for acute/chronic HBV infection as the main, sub, or third diagnosis code between 2011 and 2020. Since the calculation for liver-related deaths among HBV-infected patients was limited to those who were receiving linkage-to-care, we adjusted the total number of liver-related deaths in HBV-infected patients using the linkage-to-care rate. The data for HBV-infected patients from the NHIS database were linked to the KOSTAT database to classify the causes of death.
Definition of indices in HCV infection
The incidence of HCV infection was calculated using the KDCA infectious disease surveillance data from 2018 to 2020; the data of those with two or more claims for the corresponding diagnostic code within 3,650 days before the first report date (from 3,710 days to 60 days before report date) were excluded.
The linkage-to-care among those with HCV infection was calculated as the number of patients with two or more national health insurance claims divided by the estimated number of HCV-infected patients. The number of anti-HCV positive patients (aged ≥10 years) was calculated based on the Korea National Health and Nutrition Examination Survey data (2018–2020). The number of HCV RNA-positive patients was estimated by multiplying a reported proportion of HCV RNA positivity by the anti-HCV positivity rate [21]. Patients in linkage-to-care referred to those aged ≥10 years, with two or more national health insurance claims for HCV infection as the main, sub, or third diagnosis code between 2018 and 2020.
The treatment rate was defined as the number of HCV-infected patients prescribed with antiviral drugs out of the estimated number of HCV-infected patients that required treatment. The antiviral treatment included direct-acting antivirals and interferon-based therapies. Those who were treated referred to patients who were prescribed with antiviral drugs within 1 year after reporting to the KDCA as a newly diagnosed HCV infection case using the KDCA infectious disease surveillance data and the NHIS claims data.
HCV-related mortality was defined as the number of liver-related deaths caused by K70–76 and C22 among people with HCV infection that occurred in the year/standard population of the year. The HCV-infected patients were identified by counting those who had two or more national health insurance claims for acute/chronic HCV infection as the main, sub, or third diagnosis code between 2011 and 2020. Since the calculation for liver-related deaths among HCV-infected patients was limited to those who were receiving linkage-to-care, we adjusted the total number of liver-related deaths in HCV-infected patients using the linkage-to-care rate. The data for HCV-infected patients from the NHIS database were linked to the KOSTAT database to classify the causes of death.
Statistical analysis
Descriptive statistics were used to estimate the diagnosis, linkage-to-care, and treatment rates. The total population was based on the resident population registered in that year. Crude values were used to analyze the liver-related mortality rates. The values for 2018–2020 were calculated as the mean values for each year. The incidence and mortality rates were expressed as the number of cases per 100,000 population, while the linkage-to-care and treatment rates were expressed as percentages. Statistical analyses were performed using SPSS (version 21; IBM Co., Armonk, NY, USA) and SAS (version 9.4; SAS Institute, Cary, NC, USA) software.
RESULTS
Annual incidence of acute HBV infection
According to the data reported to the KDCA from 2018 to 2020, 356–377 patients were annually diagnosed with acute HBV infection (Fig. 1A and Supplementary Table 2). The average incidence rate was 0.71 cases per 100,000 population (range: 0.64–0.78). The incidence of acute HBV infection was significantly higher in men than in women (0.96 vs. 0.47), and the highest among those in their 20s (1.10), followed by those in their 40s (0.98), 50s (0.91), and 30s (0.88).
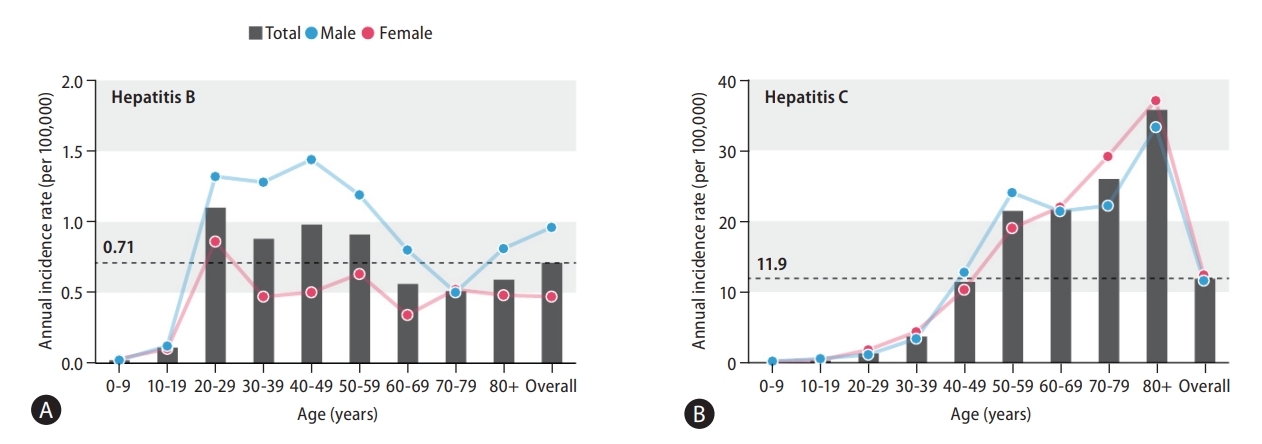
Incidence of hepatitis B and C virus infection according to age and sex. (A) Acute hepatitis B virus infection incidence in 2018–2020. This was analyzed by linking the national health insurance claims data between 2002 and 2020 based on the data of patients diagnosed with acute hepatitis B between 2018 and 2020 reported to the KDCA, excluding the data of those with two or more claims for acute hepatitis B within the 10-year wash-out period. (B) Incidence of newly detected hepatitis C virus infection in 2018–2020. This was analyzed by linking the national health insurance claims data between 2002 and 2020 based on the data of patients diagnosed with acute hepatitis C between 2018 and 2020 reported to the KDCA, excluding the data of those with two or more claims for hepatitis C virus infection within the 10-year wash-out period. KDCA, Korea Disease Control and Prevention Agency.
Linkage-to-care rate and treatment rate of HBV infection
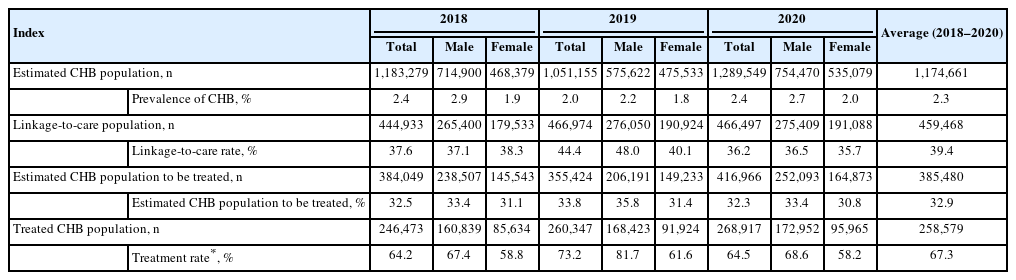
The estimated mean number of individuals infected with HBV was 1,174,661 (range: 1,051,155–1,289,549) from 2018 to 2020, according to the HBsAg positivity based on the KNHANES data. The HBsAg prevalence rate was 2.3% (2.0–2.5%), and was higher in men than women.
The linkage-to-care rate, referring to individuals who received medical care for HBV infection twice or more from 2018 to 2020, was 39.4% (Fig. 2A and Table 1). No significant difference was found between men and women in linkage-to-care; by age, the proportion of linkage-to-care patients in their 70s was the highest (55.8%), followed by those in their 60s (50.5%) and those in their 80s (46.4%) (Supplementary Table 3). Meanwhile, the proportion of linkage-to-care patients aged ≤40 years was the lowest (26.7%).

Cascade of care for hepatitis B and C virus infection. (A) Hepatitis B. (B) Hepatitis C. HCV, hepatitis C virus; HBsAg, hepatitis B virus surface antigen. *The number of newly diagnosed HCV infections represents the annual average for the 2018–2020 period.
Linkage-to-care and treatment rate of chronic hepatitis B
For the treatment rate, we first calculated the proportion of liver cirrhosis and hepatocellular carcinoma among the HBV-infected patients. In the NHIS claims data, patients with liver cirrhosis and those with hepatocellular carcinoma claims between 2018 and 2020 accounted for 8.9% and 4.3%, respectively, of the total estimated people with HBV infection according to the KNHANES data (data were not shown). Using the above proportions, the estimated number of patients with chronic hepatitis B eligible for treatment was 32.9%. As a result, the estimated treatment rate of patients with HBV infection among the those indicated to antiviral therapy was 67.3%, while the treatment rate among all patients with HBV infection, regardless of therapeutic indication, was 22.2% (Fig. 2A and Table 1). The treatment rate was the highest among those in their 50s (73.9%), followed by those in their 60s (70.5%) and those in their 40s (70.0%) (Supplementary Table 4).
Liver-related mortality of HBV infection
The average annual liver-related mortality rate of HBV infection for 2018–2020 was 18.85 cases per 100,000 population. The liver-related mortality of HBV infection peaked at 21.35 cases per 100,000 population in 2014, but eventually decreased to 17.94 cases per 100,000 population in 2020. The liver-related mortality rate, adjusted for the linkage-to-care rate, was reduced by 13.3% in 2020 compared to 2015 (Table 2). By age, the liver-related mortality rate decreased from 2011 to 2020 among those in their 40s, 50s, and 60s, but the downward trend was not remarkable among those aged ≥70 years. By sex, the liver-related mortality rate was 28.46 cases per 100,000 population in 2020 among men, which was fourfold higher than that among women (6.91 cases per 100,000 population) (Supplementary Table 5). The all-cause of annual mortality rate related to HBV infection remained stable, from 31.03 cases per 100,000 population in 2015 to 31.37 cases per 100,000 population in 2020 (Supplementary Table 6). The most frequent cause of death among HBV-infected patients was liver cancer (54.1%), followed by other infections (5.7%), accidental death (3.8%), lung cancer (3.2%), and liver cirrhosis (3.1%) (Supplementary Table 7).
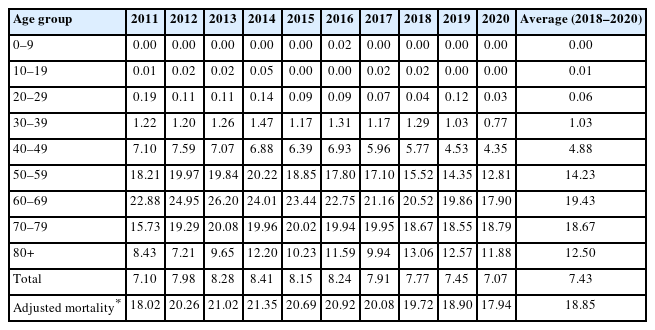
Liver-related annual mortality rate due to HBV (per 100,000 persons)
Annual incidence of HCV infection
All cases of newly detected HCV infection were reported from June 2017. Among patients who were reported to the KDCA from 2018 to 2020, the number of newly diagnosed HCV infection patients was based on the NHIS data, excluding those who had been treated for HCV infection in the last 10 years as of the reporting date; hence, an incidence rate of 11.9 cases per 100,000 population was obtained (Fig. 1B). Annually, the number of HCV-infected patients gradually decreased from 6,596 in 2018, to 6,211 in 2019 to 5,713 in 2020; the annual incidence also decreased from 12.7 to 12.0 and 11.0 cases per 100,000 population for the same period (Table 3). However, the annual incidence of HCV infection was slightly higher in women than in men and increased with age (Supplementary Table 8).

Linkage-to-care and treatment rate of hepatitis C
Linkage-to-care rate and treatment rate of HCV infection
Based on the anti-HCV positivity reported in the KNHANES by age and sex, the estimated mean number of anti-HCV positive population was 297,330 (range 273,754 to 327,432) in South Korea with a prevalence rate of 0.57% (Table 3). On the contrary, 86,212 to 102,970 people were HCV RNA-positive based on the HCV RNA positivity rate by age.
The linkage-to-care rate, defined as the HCV RNA-positive patients who had received medical care twice or more for HCV infection within the year, was 65.5% (Fig. 2B and Table 3). No significant difference was observed in the linkage-to-care rate between men and women.
The treatment rate among those diagnosed with HCV infection was 56.8% (54.9–58.7%) (Fig. 2B and Table 3). It was higher in women than in men, but the result was not significant (Supplementary Table 9). The treatment rate was the highest among those in their 50s (66.7%), followed by those in their 40s (64.6%), 20s (63.2%), and 60s (62.3%). Patients aged ≥80 years showed the lowest treatment rate (20.0%), followed by teenagers (43.9%).
Liver-related mortality rate in patients with HCV infection
The average annual liver-related mortality rate of HCV infection for 2018–2020 was 2.02 cases per 100,000 population, showing an overall downward trend. The liver-related mortality, adjusted for the linkage-to-care rate, decreased by 23.0%, from 2.35 cases in 2015 to 1.81 cases in 2020 (Table 4). By age, the liver-related mortality rates per 100,000 population in 2020 were 0.19 cases for those in their 40s, 1.20 for those in their 50s, 2.28 for those in their 60s, 4.81 for those in their 70s, and 8.08 for those in their 80s; this finding suggested that the liver-related mortality rate among people aged ≥70 years was relatively high. By sex, the liver-related mortality rate in 2020 was 2.37 cases per 100,000 population among men, which was nearly two-fold higher than that in women (1.18 cases) (Supplementary Table 10). The all-cause of annual mortality rate associated with HCV infection reduced from 4.76 per 100,000 in 2015 to 4.03 in 2020 (Supplementary Table 11). The most frequent cause of death in HCV patients was hepatocellular carcinoma (37.9%), followed by other infections (7.5%), accidental death (5.1%), liver cirrhosis (4.1%), and pneumonia (3.0%) (Supplementary Table 12).

Liver-related annual mortality rate due to HCV (per 100,000 persons)
Summary of core indicators of HBV and HCV infections in South Korea
The core indicators (annual incidence, linkage-to-care, treatment, and liver-related mortality rates) of HBV and HCV infection for validation of viral hepatitis elimination in South Korea are summarized in Table 5.
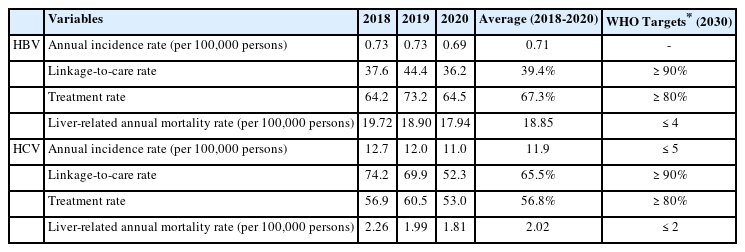
Summary of core indicators of HBV and HCV in South Korea
DISCUSSION
In this study, we analyzed the indicators for validating HBV and HCV infection elimination, which can serve as a basis for establishing strategies to achieve the WHO goal of eliminating viral hepatitis. According to data from 2018–2020, the incidence of HBV-infected in South Korea was 0.71 cases per 100,000 population, while the linkage-to-care rate, represented by the number of patients who had access to medical care out of the estimated HBV infection patients, was only 39.4%. The treatment rate was 67.3%, which failed to meet the WHO programmatic target of 80% of people diagnosed with HBV infection. The annual liver-related mortality rate due to HBV was 18.85 cases per 100,000 population, which was higher than the WHO target of 4; the most frequent cause of death was liver cancer (54%). The incidence of HCV infection in South Korea was 11.9 cases per 100,000 population, which was higher than the WHO impact target of 5. In the case of HCV infection, the linkage-to-care rate was 65.5%, while the treatment rate was 56.8%; they failed to meet the 90% and 80% targets, respectively. The annual liver-related mortality caused by HCV infection was 2.02 cases per 100,000 population, which was slightly higher than the WHO target of 2.
Meanwhile, the WHO set a global goal of reducing HBV infection incidence by 95% in 2030, compared with that in 2015. Regarding the elimination validation impact indicators, the target HBsAg positivity rates were set to 0.1% or less and 90% or more after three doses of the hepatitis B (HepB3) vaccine in children aged ≤5 years [6]. According to the national health statistics, the prevalence of HBV infection, represented by the HBsAg positivity rate, has been decreasing in South Korea after the introduction of the national vaccination and perinatal HBV infection prevention programs. In particular, the HBsAg positivity rates among Korean teenagers during 2018–2020 were 0.1% (0.1% in 2018, 0.0% in 2019, and 0.2% in 2020) [22]. The coverage rates of the HepB3 vaccine against perinatal infection prevention were 97.4% in 2017, 97.2% in 2018, and 97.8% in 2019 [23]. These results seemed to meet the WHO targets—an HBsAg prevalence of <0.1% and an HepB3 coverage rate of ≥90% in those aged 5 years and younger. This study analyzed the incidence of acute HBV infection by linking the KDCA data and the national health insurance claims data while improving the accuracy and setting a 10-year wash-out period from the reporting date. The average incidence rate remained at 0.71 cases per 100,000 population. To reduce the HBV infection incidence, in addition to continue implementing the national vaccination and perinatal infection prevention programs, oral antiviral drugs such as tenofovir should be administered at 24–32 weeks of pregnancy for mothers with high serum HBV DNA concentrations (≥200,000 IU/mL), and vaccination should be recommended to adults who have not been vaccinated or high-risk groups to prevent the occurrence of acute hepatitis B in adults. Hepatitis control measures should be prepared for groups with a high prevalence of hepatitis B, such as foreign workers, immigrants, and North Korean defectors.
The WHO suggests the HBV infection diagnosis rate as the number of patients diagnosed with HBV infection [6]. In South Korea, HBsAg screening tests are conducted in conscription tests and general health screenings conducted at the age of 40 years; however, it is difficult to calculate the diagnosis rate of hepatitis B, which represents the entire age, only with this data. In this study, the linkage-to-care rate, defined as the number of patients who had access to medical care out of the estimated number of HBV-infected patients, determined based on the HBsAg positivity rate, was calculated as a substitute for the diagnosis rate. The linkage-to-care rates were 37.6% in 2018, 44.4% in 2019, and 36.2% in 2020; the average linkage-to-care rate between 2018 and 2020 was 39.4%, which indicated that nearly 60% of the patients did not receive appropriate care. In particular, the linkage-to-care rate was lower in patients aged ≤40 years; this finding implied that many young people do not start medical care since they are in the “immune tolerant” or “gray zone” based on the current treatment guidelines. Hence, it is necessary to establish an appropriate management linkage system for infected persons after screening for hepatitis B, which is being implemented in South Korea, to improve public awareness and to strengthen education for primary healthcare workers.
The HBV treatment rate was calculated by estimating the number of HBV-infected patients aged ≥10 years based on the HBsAg positivity rate reported in the KNHANES survey (2018–2020) according to the current treatment guidelines. We analyzed the findings of Lim et al.’s study and found that 25% of chronic hepatitis B patients, 88% of cirrhotic patients, and 100% of liver cancer patients required treatment [20]. The treatment rates were reported to be 64.2% in 2018, 73.2% in 2019, and 64.5% in 2020; the average treatment rate between 2018 and 2020 was 67.3%, which failed to meet the WHO elimination validation criteria of 80% or higher. Since the national treatment guidelines have more strict criteria for selecting those eligible for treatment compared with the international guidelines, this treatment rate may be overestimated, considering that the treatment rate in all the HBV-infected patients was only 22.2% on average.
Meanwhile, the GHSS set a goal to reduce the liver-related mortality rate in HBV infection patients by 65% in 2030 or a target annual mortality rate of ≤4/100,000. The liver-related mortality rate of HBV infection patients peaked at 20.69 cases per 100,000 population in 2015, eventually decreasing to 17.94 cases in 2020; the liver-related mortality rate decreased by 13.3% from 2015 to 2020. However, this was still four to five times higher than the WHO elimination validation target of 4 cases or less per 100,000 population. Notably, the mortality rate among those in their 50s and 60s was relatively high a decade ago; recently, those in their 60s and 70s showed a higher mortality rate, and the rate was four times higher in men than in women. The most frequent cause of death was liver cancer (54.1%). The antiviral treatment for HBV suppresses the progression of liver cirrhosis to liver cancer, and leads to a lower mortality rate by suppressing the viral infection [24,25]. However, the current guidelines recommend monitoring without antiviral treatment for those in the immune tolerant phase or gray zone, even if the HBV DNA concentration is high [26-29]. One recent study evaluated that a significant number of patients who belonged to the serological IT phase were not in the histologic IT phase [30]. In another study published in South Korea, people with chronic HBV infection, with HBeAg positivity, and without cirrhosis were at the highest risk of developing liver cancer when the HBV DNA concentration is 5–5.99 log10IU/mL at the initiation of antiviral treatment. Therefore, the early initiation of antiviral treatment may reduce the risk of developing liver cancer [31]. Another study analyzed the treatment rate, the number of patients who are expected to receive treatment by 2030, cost-effectiveness, liver cancer incidence, and mortality risk under different scenarios. As a result, when the number of patients eligible for treatment increased, the cure rate increased by 12%, the incidence of liver cancer decreased by 23%, and the mortality risk was reduced by 35%, while simplifying and expanding treatment eligibility for CHB would save many lives and be highly cost-effective compared to the current treatment guidelines [20]. In order to establish a strategy to increase the number of patients eligible for treatment according to the HBV DNA concentration and ALT level, the treatment guidelines should be revised through discussions with academic and related experts. In addition, the government should expand the scope of medical care benefits for antiviral drugs, and devise measures for the early diagnosis and appropriate follow-up of patients by promoting national liver cancer screening.
The incidence of HCV infection was estimated by linking the KDCA infectious disease surveillance data and the national health insurance claims data. In the 2017–2021 KNHANES, HCV antibodies were detected in 0.7% of the general population [32]. In this study, we estimated that the incident case numbers of HCV infection were 6,596 cases in 2018, 6,211 cases in 2019, and 5,713 cases in 2020; the incidence rates per 100,000 population were 12.7 cases in 2018, 12.0 cases in 2019, and 11.0 cases in 2020, thus showing a downward trend. According to the fact sheet published by the Korean Association for the Study of the Liver, the annual incidence rate was 17.2 as of 2019 [33,34]. However, the annual incidence rate in this study was 11.9. This discrepancy probably resulted from the wash-out period in this study being set to 10 years. However, it was not sufficient to meet the WHO target of 5 cases or less per 100,000 population. Currently, there is no effective vaccine for HCV infection, but it can be cured by more than 95% when treated with direct-acting antivirals (DAAs) for 8–12 weeks. Therefore, a “prevention through treatment” strategy would be effective by curing patients infected with HCV using antiviral therapies to reduce the incidence of new viral hepatitis [35-39]. The infection control strategies in medical institutions should be strengthened while strictly regulating unsanitary tattooing or acupuncture practices.
In South Korea, the linkage-to-care rate in HCV infection patients was 65.5% between 2018 and 2020, which was lower than the WHO validation target of 90%. The link-caring rate has fallen from 74.2% in 2018 and 69.9% in 2019 to 52.3% in 2020, which seems to be attributed to the limited access to medical care due to the coronavirus disease 2019 pandemic. A total of 3,752 patients with HCV infection were treated in 2018, 3,760 in 2019, and 3,027 in 2020; and the treatment rates were 56.9% in 2018, 60.5% in 2019, and 53.0% in 2020. The overall treatment rate between 2018 and 2020 was 56.8%, which was significantly lower than the WHO validation target of 80%. Since most patients with HCV infection remain asymptomatic, an HCV infection screening should be conducted to ensure timely diagnosis and proper treatment. Since the introduction of DAAs, the cost-effectiveness of HCV infection screening has been consistently reported in the studies conducted on the Korean population [40-44]. Therefore, the diagnosis rate for asymptomatic people with HCV infection should be increased by introducing HCV screening tests as part of the national health examination and improving the treatment rate by strengthening the referral system. More importantly, effective screening strategies and referral programs should be prepared for high-risk groups (PWIDs, prisoners, HIV-infected, etc.), vulnerable groups (North Korean defectors, immigrants, foreign workers, etc.), and residents of vulnerable areas (mountainous, island areas, etc.).
The liver-related mortality of HCV infection in South Korea has been decreasing: 2.35 cases per 100,000 people in 2015, 2.53 in 2016, 2.52 in 2017, 2.26 in 2018, 1.99 in 2019, and 1.81 in 2020, with an average decrease of 23.0% between 2015 and 2020. This result may meet the WHO target of reducing 2 cases or less per 100,000 population by 2030. By age, the mortality rates per 100,000 people in 2020 were 0.19 in people in their 40s, 1.20 in their 50s, 2.28 in their 60s, 4.81 in their 70s, and 8.08 in their 80s and older; this finding showed that the liver-related mortality among older adults aged 60 years or older was relatively high. The most common cause of death was liver cancer (37.9%). The antiviral treatment for HCV infection reduces the mortality risk by preventing the progression of liver cirrhosis and the development of HCC [45,46]. In this regard, the key strategy to lower the HCV infection-related mortality is to enhance the diagnosis and treatment of those infected with no symptoms. As mentioned above, it is necessary to introduce HCV infection screening tests, establish a referral system for infected people, support expensive treatment costs, and expand treatment to older adults, high-risk groups, and vulnerable groups. To ensure an early diagnosis of liver cancer, which is the most frequent cause of death, national liver cancer screening should be more strongly promoted.
The present study has several limitations. First, regarding the treatment rate for hepatitis B, patients who are uninsured and prescribed HBV antiviral agents were not included in our analysis, as the data source for our study was from the National Health Insurance Corporation. However, we included only the estimated population who may require treatment.
Therefore, our results reflect only a proportion of patients receiving actual treatment among those who require it. Another issue was that it is difficult to accurately evaluate the number of patients who require treatment. Moreover, any health insurance coverage criteria changes could impact the number of treated individuals. Second, there were limitations in estimating the number of HCV RNA-positive individuals. While the prevalence of HCV antibody positivity is surveyed annually in the KNHANES, there is no regular testing for HCV RNA positivity. The only available data we could reference was the HCV RNA positivity rate tested temporarily from 2012 to 2015, which could have limited the accuracy due to the temporal differences. Third, the diagnosis rate presented by the WHO and the linkage-to-care rate reported in this study have different definitions from the WHO criteria. Linkage-to-care rate is a more important factor, considering that it implies continuous care of patients with the disease; however, it is likely lower than the diagnosis rate. Moreover, in this study, the linkage-to-care and treatment rate trends were difficult to predict, as only the data obtained in 2018–2020 were used. On the contrary, the mortality rate was estimated based on the 10-year data (2011–2020) to increase reliability. The last and the most significant limitation of our study is that the data source was processed. Although we calculated the incidence, diagnosis, treatment, and liver-related mortality rates for the WHO elimination target, continuous data that perfectly matched the indicators were unavailable. Therefore, we processed and estimated available data sources to produce the data. Although this was essential to obtain the data, it could affect the accuracy. To improve the accuracy of our analysis, we selected large-scale data as sources to reflect the status of South Korea and set the wash-out period to 10 years. Despite these limitations, this study is still significant in that it provides a large-scale data analysis, linking the data of KDCA, KNHANES, and NHIS and those of KOSTAT.
In summary, the core indicators of HBV and HCV infection in South Korea and the WHO’s elimination validation indicators are summarized in Table 5. As for HBV infection, the linkage-to-care, treatment rate, and liver-related mortality rates did not meet the WHO validation criteria. Therefore, the linkage-to-care rate of diagnosed patients should be increased by strengthening the follow-up management of the currently implemented HBV screening test; moreover, to reduce the mortality rate, the incidence of liver cancer and progression of liver disease should be prevented by increasing the treatment rate and expanding the eligibility criteria for treatment. As for HCV infection, the incidence, linkage-to-care, and treatment rates reported in this study did not meet the WHO validation targets. Unfortunately, there are no existing data on the incidence of HCV infection and syringe/syringe exchange among PWIDs in South Korea. Within this context, the government needs to establish a strategy to introduce the HCV infection screening test as part of the national examination to increase the diagnosis rate for asymptomatic HCV infection patients; moreover, the new HCV infection rates and HCV infection-related mortality rates should be reduced by treatment with oral DAAs. In conclusion, many of the core indicators for HBV and HCV infection identified in South Korea did not satisfy the criteria for viral hepatitis elimination validation by the WHO. Therefore, a comprehensive national strategy should be developed to eliminate hepatitis, continuously monitoring the hepatitis elimination validation targets in South Korea.
Notes
Authors’ contribution
I.H.K. designed the study; C.H.L., G.H.C., H.Y.C., S.J.H., E.S.J., Y.E.C., and Y.C. collected and analyzed the data; I.H.K., C.H.L. and G.H.C. drafted the manuscript; K.A.K., D.Y.K., H.J.Y., H.L.K., S.H.J., and I.H.K. supervised the study; all authors reviewed the manuscript.
Conflicts of Interest
The authors have no conflicts to disclose.
Acknowledgements
This research was supported by the “Korea Disease Control and Prevention Agency” research project (project No. 20211214EC3-00 and 2020-E5104-02). This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Science, ICT & Future Planning(2021R1C1C1003181).
SUPPLEMENTAL MATERIAL
Supplementary material is available at Clinical and Molecular Hepatology website (http://www.e-cmh.org).
Operational definition
Annual incidence rate of acute hepatitis B according to age, sex, and year (per 100,000 persons)
Linkage-to-care rate of hepatitis B according to age, sex, and year
Treatment rate of hepatitis B according to age, sex, and year
Liver-related annual mortality rate due to HBV by gender (per 100,000 persons)
All-cause of annual mortality rate due to HBV (per 100,000 persons)
Cause of death among patients with hepatitis B
Annual incidence rate of hepatitis C according to age, sex, and year (per 100,000 persons)
Treatment rate of hepatitis C according to age, sex, and year
Liver-related annual mortality rate due to HCV by gender (per 100,000 persons)
All-cause of annual mortality rate due to HCV (per 100,000 persons)
Cause of death among patients with hepatitis C
Abbreviations
WHO
World Health Organization
NHIS
National Health Insurance
KDCA
Korea Disease Control and Prevention Agency
KOSTAT
Statistics Korea
HBV
hepatitis B virus
HCV
hepatitis C virus
GHSS
Global Health Sector Strategy
HBsAg
hepatitis B virus surface antigen
PWID
persons who inject drugs
DALY
disease-adjusted life year
KNHANES
Korea National Health and Nutrition Examination Survey
ICD-10
International Classification of Diseases 10th Revision
ALT
alanine aminotransferase
DAAs
direct-acting antivirals
References
Article information Continued
Notes
Study Highlights
• WHO published the interim guidance for country validation of viral hepatitis elimination, which sets impact targets and programmatic targets.
• The many indicators identified in the Korean population, including incidence rates, linkage-to-care, treatment, and liver-related mortality, did not satisfy the WHO criteria for validation of viral hepatitis elimination.
• A comprehensive national strategy should be developed to eliminate hepatitis infection in South Korea.