

INTRODUCTION
Liver disease is an important cause of death worldwide, and is very prevalent in Asian countries. Chronic liver disease including liver cirrhosis ranked as the 12th cause of mortality in the United States in 20091 and the 8th cause of death in South Korea in 2010. The mortality rate due to chronic liver disease in Korea was reported as 13.8 per 100,000 population with the peak mortality in middle-aged males, suggesting a heavy disease burden on family and society.2 Moreover, liver cancer is the 4th common cancer and the 2nd highest cancer mortality in Korean males.2 The socioeconomic costs of liver disease, especially direct medical costs, rapidly increased from 2004-2008.3
The type and cause of liver disease differs geographically and changes dynamically according to the socioeconomic changes and vaccination programs. It is important to have this information to determine the priorities for healthcare policy and research. However, the types and causes of the whole spectrum of liver disease have not been reported in Korea, which should be helpful for the estimation of the disease burden and changing trend of liver disease.
This study aimed to describe the current type and cause of liver disease in a Korean cohort of 6,307 patients who visited a liver clinic of a community hospital from 2005-2010.
MATERIALS AND METHODS
Patients
A total of 8,701 patients presented to a liver clinic of Seoul National University Bundang Hospital (SNUBH, a secondary community hospital during the study period) from April, 2005 to May, 2010 because of the liver problems. All of the patients who appeared in the outpatient clinic or were hospitalized were included in the database, which was prospectively updated every week during the study period. Among them, 1,443 patients were excluded because they visited the clinic only once without further follow-up, therefore the diagnosis could not be confirmed. Most of the patients brought previous medical records and were reassured about their minor problems without undertaking the confirmatory diagnostic tests. In the remaining 7,258 patients who visited the clinic at least two times and proceeded to a diagnostic work-up, 924 patients were excluded because they were confirmed to have non-liver related problems such as gallstones or gastrointestinal problems, and 27 patients were excluded because of uncertain diagnosis after initial examinations. Therefore, the subjects of this study included 6,307 patients who had various liver diseases according to the consistent diagnostic criteria set and maintained by an experienced hepatologist (SHJ).
Methods
The diagnostic criteria for acute hepatitis was at least a 5-fold elevation of serum alanine aminotransferase (ALT) level without a history of previous liver disease and <6 months of disease duration. Acute hepatitis was classified as viral hepatitis caused by hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis E virus (HEV), and Epstein-Barr virus (EBV), toxic hepatitis, and acute cryptogenic hepatitis. Toxic hepatitis was diagnosed according to the compatible clinical data to RUCAM (Russel Uclaf Causality Assessment) with adequate exclusion of other causes of acute liver disease.
The diagnosis of chronic hepatitis was made on the basis of the abnormal liver function test or carriage of hepatitis virus without evidence of cirrhosis, which was classified as viral hepatitis, alcoholic liver disease (ALD), nonalcoholic fatty liver disease (NAFLD), autoimmune liver disease, Wilson disease, and others. The diagnosis of ALD was based on the documentation of excessive alcohol consumption more than 60 g/day and evidence of liver disease. The diagnosis of NAFLD was based on the following criteria: (1) absence of clinical or serologic evidence of HBV or HCV infection; (2) alcohol consumption <20 g/day; (3) exclusion of other liver disease such as autoimmune hepatitis, drug-induced hepatitis, hemochromatosis, Wilson disease, primary biliary cirrhosis, primary sclerosing cholangitis; intestinal bypass surgery, and (4) radiological findings of fatty liver, which included hepatomegaly, diffuse increase in echogenicity of the liver parenchyma, and vascular blunting on ultrasound or the ratio of liver density-to-spleen density, measured in Hounsfield Units, was less than 1.0 on computed tomography (CT).
Liver cirrhosis was diagnosed by presence of evidence of portal hypertension manifested as varices, splenomegaly, ascites, or portosystemic encephalopathy, and compatible imaging findings accompanied by thrombocytopenia (<120,000/uL). Liver cirrhosis was classified as viral cirrhosis, alcoholic cirrhosis, cryptogenic cirrhosis, and cirrhosis related to autoimmune liver disease or Budd-Chiari syndrome.
Hepatocellular carcinoma (HCC) was diagnosed according to the 2009 criteria of the Korean liver cancer study group.4 For the clinical diagnosis of HCC, presence of risk factors such as HBV or HCV infection or liver cirrhosis and elevated serum alpha fetoprotein (AFP) over 200 ng/mL, with typical imaging findings of HCC on either dynamic CT or magnetic resonance imaging (MRI), were required. In the presence of risk factors and serum AFP level <200 ng/mL, at least two imaging studies should be typical among dynamic CT, MRI, or hepatic artery angiography for the diagnosis of HCC. If the clinical diagnosis was uncertain, pathologic diagnosis of HCC was required. The cause of HCC was classified as viral HCC, alcoholic HCC, and cryptogenic HCC. Alcoholic cause was defined as the consumption of at least 60 g of ethanol per day for 5 years. Other mass lesions were classified as cholangiocarcinoma, metastatic liver cancer, hemangioma, focal nodular hyperplasia (FNH), angiomyolipoma (AML), cysts, pyogenic abscess, and eosinophilic abscess.
To simply the analysis, patients with multiple diagnoses were assigned to the group with the greatest acuteness and severity of disease. This meant that acute hepatitis had priority over chronic liver disease, and the hierarchy of severity of diagnostic group was arbitrarily defined as follows. Malignant tumor had the highest severity, accompanied by liver cirrhosis, and chronic hepatitis. The other benign disease group was at the lowest severity level. For example, if a patient had HBV-related cirrhosis and HCC, the diagnosis was categorized into HCC rather than cirrhosis. If a HBV carrier presented as acute hepatitis A, the diagnosis was defined as acute hepatitis rather than chronic hepatitis. If a patient visited the clinic because of hepatic solid mass on routine check-up and hepatic hemangioma was found on the initial imaging study with tiny hepatic cysts, the diagnosis was defined as hemangioma rather than cyst.
This study was approved by the Institutional Review Board of SNUBH.
RESULTS
Overall types of liver disease in the cohort of 6,307 patients
The subjects had a mean age ┬▒ standard deviation (SD) of 49.3┬▒14.2 years (range, 13-90 years). Males constituted 60.7%. The mean follow-up duration of the subjects was 496.0┬▒562.0 days (range,10-1,888 days).
The proportion of each type of liver disease is summarized in Table 1 and Figure 1. Acute hepatitis formed 8.4%, chronic hepatitis 62.7%, liver cirrhosis 12.2%, primary liver cancer 8.1%, and other diseases 8.7% of the whole cohort. Therefore, chronic liver diseases occupied 83.0% and serious complication of liver disease such as cirrhosis and primary liver cancer comprised 20.3% of the total subjects. Among the other benign diseases (n=510, 8.1%), hemangioma (n=257, 50.4%) and cystic lesions (n=166, 32.5%) were the major lesions.
Overall cause of liver disease in the cohort of 6,307 patients
The major causes of acute hepatitis were viruses in 58.5% and toxic materials in 32.4%, while 9.1% was attributed to acute cryptogenic hepatitis. Chronic hepatitis was caused by viruses in 51.2%, NAFLD in 33.3%, alcohol in 13.0%, and others in 2.3%. Cirrhosis was caused by HBV or HCV in 73.4%, alcohol in 18.1%, and others in 8.5%. HCC was caused by HBV or HCV in 86.6%, alcohol in 11.6%, and others in 1.8%.
The relative importance of hepatitis viruses as the cause of liver disease progressively increased from chronic hepatitis to cirrhosis, and to HCC, while that of NAFLD progressively decreased, if NAFLD is the main cause of cryptogenic cirrhosis and HCC (Fig. 2).
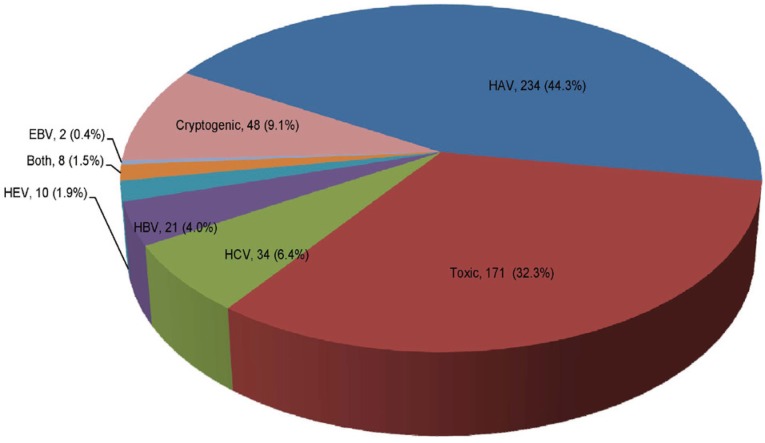
The viral causes of acute hepatitis were HAV in 44.3%, HBV in 4.0%, HCV in 6.4%, HEV in 1.9%, EBV in 0.4%, and others in 1.5%. In addition, toxic hepatitis due to various materials comprised 32.4%, and cryptogenic causes comprised 9.1% of the acute hepatitis group (Fig. 3).
Among the causes of chronic viral hepatitis, HBV occupied 82.0% and HCV occupied 17.5%, while in cirrhosis and HCC, HBV formed 83.7% and 74.9% of the viral cause, respectively (Fig. 4).
Mass lesions in liver
Among the 1,037 patients who presented with liver mass lesions, malignant tumor was diagnosed in 52.6% and benign mass lesions in 47.4%. In the malignant tumors, 88.8% were HCC, 4.6% were cholangiocarcinoma, and 6.6% were metastatic tumors from various organs. In the primary liver cancer, HCC comprised 95.1% (484/509), and cholangiocarcinoma comprised 4.9% (25/509). Among the benign mass lesions, hemangioma and cyst were diagnosed in 257 patients and 166 patients as the main liver problem, respectively. The remaining benign mass lesions included benign regenerative nodules, pyogenic liver abscess and eosinophilic liver abscess (Table 2).
DISCUSSION
In this study, we describe the current type and cause of liver disease in a single community hospital in Korea from 2005-2010. A cohort of patients who visited the liver clinic in a community hospital was consecutively enrolled and the diagnosis of all of the enrolled patients was confirmed by retrospective review of medical records. Among the total of 6,307 patients, 528 (8.4%) patients were classified as acute hepatitis, 3,957 (62.7%) as chronic hepatitis, 767 (12.2%) as liver cirrhosis, 545 (8.6%) as liver cancer, and 510 (8.1%) as benign liver mass or other diseases.
In this cohort of liver disease, the patients diagnosed as acute hepatitis comprised 8.4%; they had a mean age of 40.1 years and were slightly male in proportion (50.8%). The major cause of acute hepatitis was viruses (n=309, 58.5%), such as HAV (n=234, 44.3%), HBV (n=21, 4.0%), HCV (n=34, 6.4%), HEV (n=10, 1.9%), EBV (n=2, 0.4%), and others (n=48, 9.1%). In another study conducted in Korea, Kang et al. reported that HAV caused 56.4% of acute viral hepatitis during 2005-2006, HBV 12.7%, HCV 18.2%, HEV 9.1%.5 During 2007-2009, a nationwide outbreak of hepatitis A occurred in Korea. However, the hepatitis A cases decreased dramatically during subsequent years, because of active immunization of young adults and children.6 Our data also reflect the dynamic changes of acute viral hepatitis with time.
The next most frequent cause of acute hepatitis in the present study was toxic materials (n=171), which comprised 32.4% of acute hepatitis. The remaining 48 cases did not have any confirmed etiology, so they were classified as cryptogenic acute hepatitis, which may have included undiagnosed viral or toxic hepatitis and transient hepatitis related to other systemic diseases or unknown causes.
In this study, the most prevalent chronic liver disease was chronic hepatitis (62.7%) including viral hepatitis, NAFLD, ALD, and others. It was followed by liver cirrhosis (12.2%) and primary liver cancer (8.1%). Therefore, liver cirrhosis and HCC constituted about 20% of the overall chronic liver disease. The mean age of patients with chronic hepatitis, cirrhosis, and HCC were 47.1 years, 56.6 years, and 62.3 years, respectively. The male proportion of chronic hepatitis, cirrhosis, and HCC were 62.5%, 64.3%, and 74.8%, respectively. The male predominance was observed through the whole spectrum of chronic liver disease, especially in HCC, with a male-to-female ratio of 2.97, compared to that in liver cirrhosis (1.80).
The major cause of the overall chronic liver diseases was hepatitis virus (3009/5208, 57.8%) followed by NAFLD (1377/5208, 26.4%) and alcohol (708/5208, 13.6%), if cryptogenic cirrhosis and HCC were assumed to be burnt-out NAFLD, although the patients with cryptogenic cirrhosis and HCC may be burnt-out autoimmune hepatitis or occult HBV disease. In the viral hepatitis, HBV comprised 82.0%, 83.7%, and 74.9% of chronic hepatitis, cirrhosis, and HCC, respectively, while HCV comprised 17.5%, 15.5%, and 24.1%, respectively. The viral cause occupied a progressively increasing portion from chronic hepatitis to cirrhosis, and finally to HCC, while NAFLD occupied a progressively less portion. This finding suggests the relatively stronger carcinogenic or cirrhotic potential of hepatitis viruses compared to that of NAFLD. However, this study is not a long-term follow-up study and reports a single center experience. Therefore, further study is needed to clarify carcinogenic potential of hepatitis virus and NAFLD. According to the study of natural history of NAFLD, about 20% of NAFLD progresses to nonalcoholic steatohepatitis (NASH) and, among the cases of NASH, about 20-30% progress to cirrhosis.7 Therefore, in the overall NAFLD, about 2-3% of the patients progress to cirrhosis, while in chronic hepatitis B or C patients about 15-25% progress to cirrhosis.8,9 These data are compatible with our results.
The recent prevalence of NAFLD in Korean population was estimated as 16.1%,10 while HBV carrier rate was 2.9%,11 and HCV seroprevalence was about 1%.12 Considering the rapidly increasing prevalence of NAFLD and decreasing prevalence of hepatitis B, the type and cause of the chronic liver disease may be rapidly changing in Korea.
Autoimmune liver diseases such as autoimmune hepatitis and primary biliary cirrhosis presently comprised about 2% of the cases chronic hepatitis, and 1% of liver cirrhosis.
Benign liver tumors included mainly hemangioma and cystic diseases. Our results showed that eosinophilic liver abscess is not very rare, and FNH was more common than hepatic adenoma.
The major limitation of this study is the single center experience, which may not represent the general features of nationwide liver disease. Although our hospital was a secondary level, community hospital during the study period, referral bias may exist. The diagnostic criteria may not be perfect. Moreover, some patients have more than one cause such as viral cause and excessive alcohol consumption, but we classified those patients as viral cause, because of simplification of data analysis. In the malignant tumors, cholangiocarcinoma was found in 4.6% of the subjects, however, some patients with cholangiocarcinoma visited to the biliary specialists or oncologists, which may explain why the proportion is low reported in the other studies. However, all the criteria were predefined and consistent application of the criteria and relatively strict diagnosis of NAFLD was made by an experienced hepatologist. Despite the limitations, the study subjects were consecutively enrolled without arbitrary selection with good sample size, and the complete inclusion of the whole cohort may be a strong point of this study. Because, there have been no available data on the overall types and cause of current liver diseases encompassing such comprehensive data, the results of this study may be a useful basis for estimation of the liver disease burden and in revealing a changing trend of liver disease in Korea.
In conclusion, we describe the types and causes of the current liver disease in Korea. Further study on this subject in different hospitals may be warranted to clarify the general features of the current status of liver disease.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




