


Graphical Abstract
INTRODUCTION
Hepatitis B virus (HBV) infection is the most prevalent chronic viral infection globally and is associated with the development of liver disease, including hepatocellular carcinoma (HCC) [1-3]. HBV infection is also a recognized risk factor for non-Hodgkin lymphoma (NHL) [4,5]. Diffuse large B-cell lymphoma (DLBCL) is a common type of NHL, and a significant association between chronic hepatitis B (CHB) and DLBCL development has been reported [6]. Consequently, CHB is considered a major risk factor for DLBCL [4,5,7].
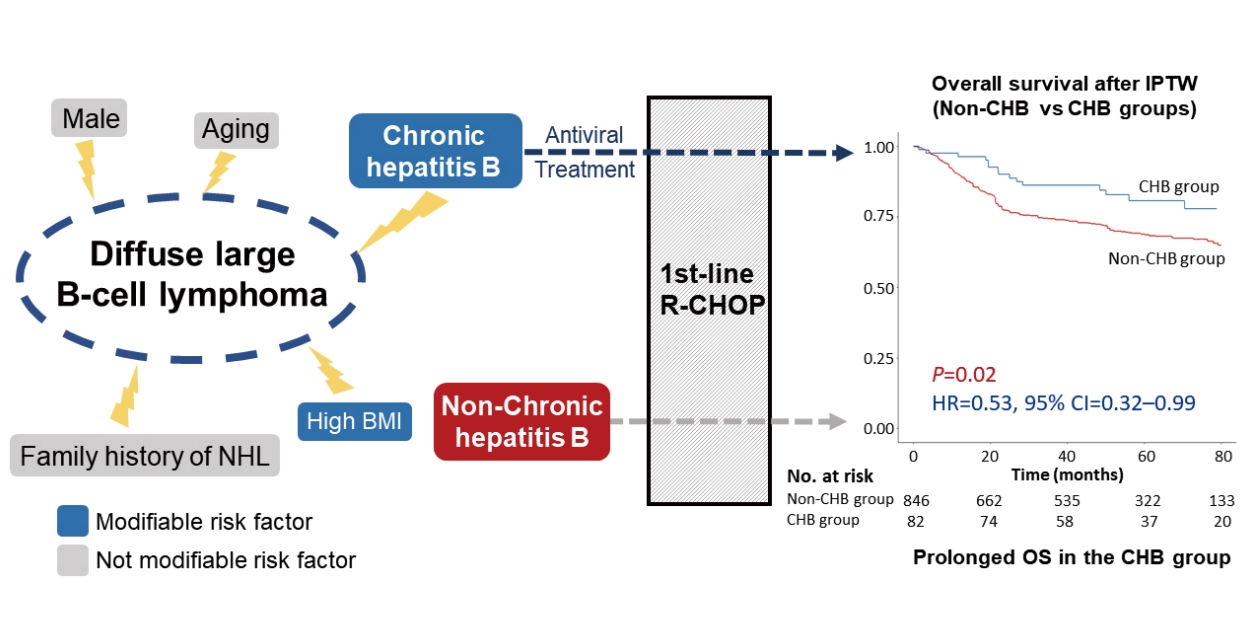
In our recent population-based study, CHB patients had an increased risk of NHL, and antiviral therapy was suggested to attenuate the risk of NHL to be comparable to that of non-CHB subjects [8]. This result supports the hypothesis that active HBV replication could contribute to NHL development in CHB patients. However, whether antiviral treatment decreases the disease progression or recurrence of HBV-associated NHL or DLBCL is debatable [4,7,9]. Several risk factors for DLBCL have been identified, including B-cell-activating autoimmune disease, hepatitis C virus (HCV) positivity, first-degree familial history of NHL, high body mass index, and HBV infection [10,11]. Many of these risk factors are not modifiable; however, HBV infection is modifiable through antiviral treatment. Thus, we hypothesized that the disease course of HBV-associated DLBCL patients may be improved with antiviral therapies, similar to patients with HBV-unassociated DLBCL resulting from other non-modifiable risk factors.
In the present study, the prognoses of HBV-associated DLBCL patients receiving antiviral treatment and of HBV-unassociated DLBCL patients were compared. All patients received rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) as first-line chemotherapy.
MATERIALS AND METHODS
Study population
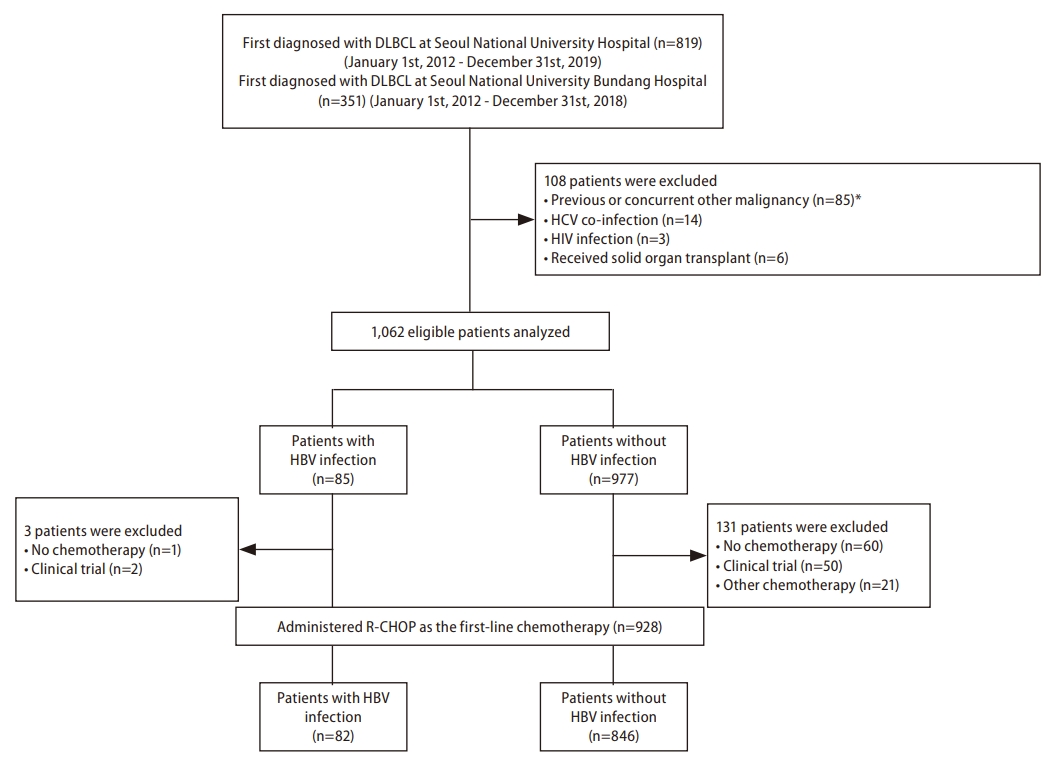
We retrospectively included patients who were first diagnosed with DLBCL and received R-CHOP treatment as first-line chemotherapy at Seoul National University Hospital (SNUH; Seoul, Korea) between January 1, 2012, and December 31, 2019, or at Seoul National University Bundang Hospital (SNUBH; Seongnam, Korea) between January 1, 2012, and December 31, 2018. DLBCL was diagnosed histologically according to the 2008 and 2016 World Health Organization classification of tumors of hematopoietic and lymphoid tissues [12,13]. The cell of origin was defined as a germinal center B cell (GCB) or non-GCB subtype based on the Hans algorithm [14]. We excluded patients who were diagnosed with other malignancies within 5 years before DLBCL diagnosis, had other, concurrent viral infections (i.e., HCV, hepatitis D virus, or human immunodeficiency virus [HIV]) or who had undergone organ transplantation. Based on the presence of hepatitis B surface antigen (HBsAg) or HBV DNA, patients were classified into either the CHB group or the non-CHB group (Fig. 1).
All DLBCL patients underwent routine serology screening including HBsAg and anti-HBV core antibody (anti-HBc) before chemotherapy to determine the risk of HBV reactivation or flare [15]. HBsAg and anti-HBc were examined using the ARCHITECT i2000SR (Abbott Laboratories, Abbott Park, IL, USA) and the Alinity i system (Abbott Laboratories), respectively. CHB patients who were already being treated with oral nucleos(t)ide analogues (NAs) continued antiviral treatment. All untreated CHB patients positive for either HBsAg or anti-HBc started antiviral treatment with an NA before initiation of rituximab according to the CHB treatment guidelines [16-19]. Prophylactic antiviral agents were discontinued 12 months after completion of R-CHOP treatment if blood tests showed continuous HBV suppression. In cases of DLBCL recurrence requiring subsequent treatment, the prophylactic antiviral agents were resumed if indications were met. In addition, therapeutic antivirals were administered if a patient experienced HBV reactivation and a hepatitis flare-up following cessation of prophylactic antivirals [17,20].
This study conformed to the ethical guidelines of the World Medical Association Declaration of Helsinki and was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. H-2205-176-1329). The requirement for informed consent from patients was waived due to the retrospective nature of the study.
Definitions and assessments
The Ann Arbor and Lugano classifications were used for DLBCL staging [21,22]. Computed tomography (CT) and positron emission tomography-CT (PET-CT) were conducted to evaluate the extent of lesions at baseline. Bone marrow biopsy was performed to confirm bone marrow involvement of DLBCL. Performance status was presented as Eastern Cooperative Oncology Group scores. The International Prognostic Index (IPI) was used to predict the outcomes for individuals receiving rituximab in combination with chemotherapy [23]. CT or PET-CT was performed every two or three cycles of R-CHOP chemotherapy to evaluate the treatment response. Additional descriptions of Ann Arbor classification and IPI risk are provided in Supplementary Tables 1 and 2, respectively. The diagnostic criteria for cirrhosis are described in Supplementary Methods.
Outcomes and follow-up
The primary endpoint was time-to-progression (TTP) of DLBCL. The secondary endpoints were tumor response, progression-free survival (PFS), and overall survival (OS). The treatment response of NHL was assessed according to the Lugano criteria as complete remission (CR), partial response, stable disease, or progressive disease [21]. The index date was defined as the date on which the patient started R-CHOP treatment as first-line chemotherapy. Patients were censored at the last date of follow-up, the date of death, or the data cut-off date (i.e., April 30, 2022), whichever came first.
After each patient completed six cycles of R-CHOP, CT or PET-CT was performed to evaluate the treatment response, and a follow-up CT or PET-CT was performed every 3 months for 1 year after the last round of chemotherapy. An annual imaging follow-up (CT or PET-CT) was performed after patients maintained CR for 1 year. When a patient experienced symptoms of disease progression, unscheduled diagnostic studies including CT or PET-CT were performed according to the decision of attending physicians.
Statistical analysis Categorical variables were presented as frequencies (%) and continuous variables as medians and interquartile ranges (IQRs). PearsonŌĆÖs Žć2 test or FisherŌĆÖs exact test was used to compare categorical variables, and StudentŌĆÖs t-test or MannŌĆōWhitney U test was used to compare continuous variables. The HolmŌĆōBonferroni method was used to control for Type I error resulting from multiple comparisons (Supplementary Methods) [24]. Inverse probability of treatment weighting (IPTW) [25] was used to reduce potential confounding. Age, sex, Ann Arbor classification, IPI risk, GCB subtype, lactate dehydrogenase level, presence of an extranodal lesion, bone marrow involvement, and cirrhosis were included in the propensity score (PS) calculation. The KaplanŌĆōMeier estimator and log-rank test were used to determine TTP, PFS, and OS. For risk factor analysis, factors found significant in univariable analysis or those with a low degree of collinearity were subjected to multivariable analysis using Cox regression analysis. P-values for interactions were used to evaluate the differential effect of current HBV infection on DLBCL clinical outcomes based on subgroups [26]. All statistical analyses were performed using R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria). P-values <0.05 were considered statistically significant.
RESULTS
Baseline characteristics
The median follow-up duration was 50.5 months (IQR=25.6ŌĆō69.7 months). The baseline characteristics of the study population are presented in Table 1. A total of 928 patients was included in this study; 82 had evidence of current CHB infection and were classified as the CHB group; the remaining 846 patients comprised the non-CHB group. After IPTW, the baseline characteristics were generally well balanced between the study groups (Table 1).
Comparison of outcomes between the CHB and non-CHB groups
The CHB and non-CHB groups had similar objective response rates (91.5% vs. 91.0%, P=1.00); however, the non-CHB group showed a greater proportion of SD or PD (1.2% vs. 6.5%, P=0.046; Supplementary Table 3).
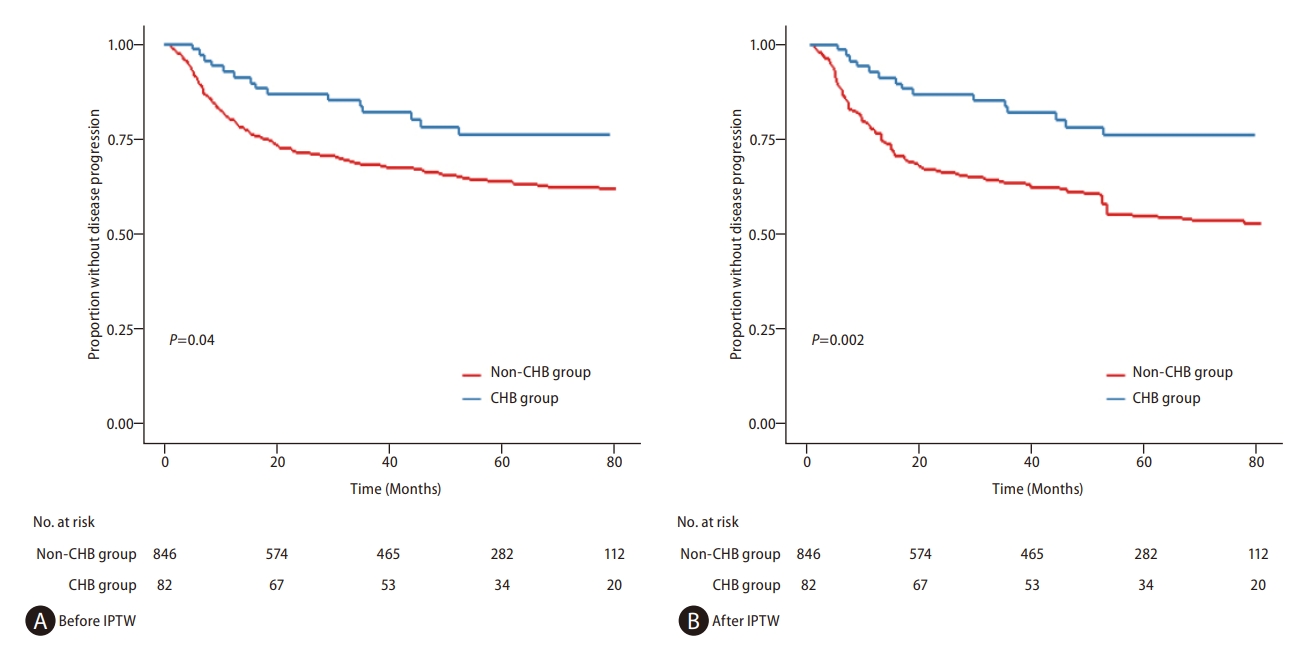
During the study period, 269 patients (29.0%) experienced tumor recurrence or DLBCL progression: 16 patients (19.5%) in the CHB group and 253 patients (29.9%) in the non-CHB group. TTP was significantly longer in the CHB group before IPTW (hazard ratio [HR]=0.58, 95% confidence interval [CI]=0.35ŌĆō0.97, log-rank P=0.04) and remained significantly longer after IPTW (HR=0.49, 95% CI=0.29ŌĆō0.82, log-rank P=0.002; Fig. 2 and Table 2). Multivariable analyses also showed longer TTP in the CHB group than the non-CHB group, both before IPTW (adjusted HR [aHR]=0.49, 95% CI=0.29ŌĆō0.82, P=0.007) and after IPTW (aHR=0.42, 95% CI=0.26ŌĆō0.70, P<0.001; Table 2). All the above results were statistically significant after the HolmŌĆōBonferroni correction for multiple comparisons (Supplementary Results). Separate analyses of the SNUH and SNUBH subcohorts yielded the same results (Supplementary Table 4). TTP was significantly longer in the CHB group after IPTW in both SNUH (HR=0.51, 95% CI=0.29ŌĆō0.92, log-rank P=0.03; Supplementary Fig. 1) and SNUBH subcohorts (HR=0.40, 95% CI=0.10ŌĆō0.94, log-rank P=0.04; Supplementary Fig. 2). In the subgroup analyses, the difference in TTP between CHB and non-CHB groups was influenced by the presence of liver cirrhosis, bone marrow involvement, IPI risk group, and GCB subtype (Supplementary Table 5A). Subgroup analyses showed no variables affecting the difference in TTP between the CHB and non-CHB groups in the SNUH subcohort; however, in the SNUBH subcohort, elevated LDH affected the difference (Supplementary Table 5B, C). Difference was not observed in TTP based on hepatitis B e antigen status in CHB patients before IPTW (HR=0.58, 95% CI=0.07ŌĆō4.43, log-rank P=0.59) and after IPTW (HR=0.63, 95% CI=0.11ŌĆō7.50, log-rank P=0.93). A low IPI risk and an early Ann Arbor stage were associated with a significantly longer TTP in the CHB and non-CHB groups both before and after IPTW (Supplementary Figs. 3 and 4).
Univariable analyses showed a significant difference in PFS between the CHB and non-CHB groups both before IPTW (HR=0.61, 95% CI=0.40ŌĆō0.94, log-rank P=0.03) and after IPTW (HR=0.53, 95% CI=0.34ŌĆō0.82, log-rank P=0.004; Supplementary Fig. 5). Multivariable analyses also showed significantly longer PFS in the CHB group than the non-CHB group both before IPTW (aHR=0.56, 95% CI=0.37ŌĆō0.87, P=0.01) and after IPTW (aHR=0.50, 95% CI=0.32ŌĆō0.77, P=0.002; Supplementary Table 6). A marginal but not significant difference in PFS was observed between the two groups after IPTW in both SNUH (HR=0.63, 95% CI=0.39ŌĆō1.02, log-rank P=0.06; Supplementary Fig. 6) and SNUBH subcohorts (HR=0.32, 95% CI=0.10ŌĆō1.04, log-rank P=0.06; Supplementary Fig. 7).
In the CHB group, OS was also significantly longer than in the non-CHB group both before IPTW (HR=0.55, 95% CI=0.33ŌĆō0.92, log-rank P=0.02; Fig. 3A) and after IPTW (HR=0.53, 95% CI=0.32ŌĆō0.99, log-rank P=0.02; Fig. 3B). Multivariable analyses indicated that the CHB group was independently associated with a longer OS than the non-CHB group both before IPTW (aHR=0.55, 95% CI=0.33ŌĆō0.93, P=0.03; Table 3A) and after IPTW (aHR=0.49, 95% CI=0.29ŌĆō0.81, P=0.007; Table 3B). Regarding liver-related deaths, 2 patients in the CHB group who had cirrhosis at baseline died: 1 due to newly developed HCC and 1 due to acute liver failure. In the sensitivity analyses that excluded these 2 patients and involved reanalysis of the data, the results for TTP remained consistent (Supplementary Results). In the non-CHB group, liver-related death did not occur, and the risk of liver failure was not significantly different between the two groups (7.1% vs. 0.0%, P=0.07; Supplementary Table 7). Non-liver-related deaths occurred less frequently in the CHB group than in the non-CHB group after IPTW (HR=0.48, 95% CI=0.27ŌĆō0.88, log-rank P=0.02; Supplementary Fig. 8). Although OS tended to be longer in the CHB group, difference was not observed between the two groups in either SNUH (Supplementary Fig. 9) or SNUBH subcohort (Supplementary Fig. 10) before and after IPTW. Lower IPI risk and early Ann Arbor stage were associated with significantly longer TTP in the CHB and non-CHB groups both before and after IPTW. A low IPI risk and an early Ann Arbor stage were also associated with significantly longer PFS and OS in the CHB and non-CHB groups both before and after IPTW (Supplementary Figs. 11ŌĆō14).
Comparisons of TTP among the CHB, resolved-HBV, and never-HBV groups
The non-CHB group was further subclassified into resolved-HBV (HBsAg-negative but anti-HBc-positive) or never-HBV (HBsAg-negative and anti-HBc-negative) groups. Within the non-CHB group, the resolved-HBV group was older, had a larger proportion of patients with cirrhosis, and had higher IPI risk scores than the never-HBV group (Supplementary Table 8). Significant difference was not observed in TTP before IPTW between the CHB and never-HBV groups (HR=0.65, 95% CI=0.39ŌĆō1.09, log-rank P=0.10). However, after IPTW, the CHB group had a longer TTP than the never-HBV group (HR=0.52, 95% CI=0.31ŌĆō0.88, log-rank P=0.01). Both before and after IPTW, significant differences were observed in TTP between the CHB and resolved-HBV groups before IPTW (HR=0.47, 95% CI=0.28ŌĆō0.80, log-rank P=0.005) and after IPTW (HR=0.43, 95% CI=0.25ŌĆō0.75, log-rank P=0.003; Supplementary Fig. 15). TTP was similar between never-HBV and resolved-HBV patients after IPTW (HR=1.12, 95% CI=0.88ŌĆō1.53, log-rank P=0.30).
DISCUSSION
In this study, we examined the clinical outcomes of DLBCL patients treated with R-CHOP based on the HBV infection status. After baseline characteristics were balanced with IPTW, patients with CHB had a 51ŌĆō58% lower risk of progression. In addition, the CHB group showed longer PFS and OS than the non-CHB group. When the non-CHB group was subdivided into the resolved-HBV or never-HBV groups, the CHB group showed significantly longer TTP than both the re-solved-HBV and never-HBV groups; however, significant difference was not observed in TTP between the resolved-HBV and never-HBV groups. In subgroup analysis, the results were comparable between SNUH and SNUBH subcohorts.
Prior to the development of antivirals, many HBsAg-positive lymphoma patients died of severe hepatitis caused by HBV reactivation [15]. The risk of HBV reactivation during chemotherapy for lymphoma is significantly reduced by antiviral prophylaxis [27]. Consequently, current practice guidelines advocate antiviral prophylaxis for patients being treated with chemotherapeutic agents, particularly rituximab [16,18]. Clinical and epidemiological evidence further supports an association of HBV with DLBCL development [6,8]; however, the extrahepatic effect of HBV suppression by NAs on HBV-associated DLBCL remained unknown. Our study shows that current HBV infection is a favorable prognostic factor for DLBCL patients in the era of antiviral prophylaxis.
Multiple mechanisms may explain why antiviral treatment can prolong TTP. First, reducing HBV viral load inhibits HBV-driven antigen stimulation of B cells, inhibiting lymphoma progression or recurrence [28]. In the majority of HBsAg-positive DLBCL patients, the third complementarity-determining region of heavy- or light-chain sequences displayed high homology to antibody-targeting HBsAg [28], indicating that these DLBCL cells originated from B cells reactive to HBV due to chronic HBV antigen stimulation. If persistent HBV-driven antigen stimulation is a primary cause of DLBCL development, then blocking antigen stimulation can inhibit one of the major proliferative and anti-apoptotic signals in HBV-associated DLBCL. Second, decreasing the HBV viral load reduces the HBV-mediated apolipoprotein B mRNA-editing catalytic polypeptide (APOBEC)-induced mutagenesis [29,30]. APOBEC3 cytidine deaminases are essential for regulating gene expression, innate immunity, and suppressing HBV infection. Aberrant expression during chronic viral infections or inflammation can cause the development of cancer [31-33]. APOBEC3 genes are significantly increased in CHB patients and may induce extrahepatic malignancy through the migration of peripheral blood mononuclear cells or lymphoid cells with upregulated APOBEC3 expression in response to HBV infection [34,35]. In a gene expression study on DLBCL patients, an association was found between APOBEC3 genes and poor prognosis, indicating these genes may contribute to the development of DLBCL [36]. Therefore, reducing HBV viral load with antiviral agents can decrease APOBEC3 expression and potentially lead to a reduction in cancer development [37]. Third, both the innate and adaptive immune systems are dysfunctional in patients with a high HBV viral load, resulting in decreased immune surveillance [38]. However, antiviral treatment restores immune surveillance of malignancy, reducing the likelihood of lymphoma recurrence [39,40].
In the subgroup analysis, the CHB group of cirrhotic patients tended to have a shorter TTP than the non-CHB group. Furthermore, the cirrhotic CHB patients did not receive significantly lower doses of chemotherapeutic agents than the non-cirrhotic patients (data not shown). However, because the progression of cirrhosis is reportedly associated with persistent active viral replication, cirrhotic HBV patients are expected to be exposed to higher viral loads than non-cirrhotic patients [41]. Consequently, cirrhotic patients may have a higher risk of prolonged HBV-mediated APOBEC-induced mutagenesis, leading to an increased mutation burden of DLBCL, which is associated with a poor prognosis. Immune dysfunction in cirrhotic patients may possibly contribute to DLBCL recurrence by reducing immune surveillance; however, further research on the underlying mechanisms is warranted [42].
The results of the present study revealed that patients with current HBV infection (i.e., HBsAg-positive) and patients with resolved HBV infection (i.e., HBsAg-negative but anti-HBcpositive) showed distinct clinical trajectories. This finding indicates that current HBV infection is a risk factor for development and recurrence of DLBCL. According to previous studies, infected HBV continuously stimulates B cells and facilitates mutagenesis, both of which lead to DLBCL development [28,43]. However, neither chronic HBV antigen stimulation nor HBV-mediated mutagenesis occurs in patients with resolved HBV infection. Therefore, antiviral therapy may have limited chemopreventive effects in patients where DLBCL development occurs through alternate pathways.
Off-target effects of antivirals may also be insufficient to explain their preventive effect on DLBCL progression or recurrence. For example, tenofovir is a potent antiviral that blocks HBV viral replication and induces interferon lambda 3 (IFN-╬╗3) production, exhibiting additional unanticipated (i.e., off-target) pharmacological effects [44]. IFN-╬╗ has antitumor effects by inducing cell cycle arrest and causing apoptosis [45,46]. If this off-target effect of antivirals plays a role in preventing lymphoma progression or recurrence, patients with resolved HBV should show a trend either similar to that of CHB patients or superior to never-HBV patients. However, resolved-HBV patients showed a trend similar to never-HBV patients. Therefore, genetic factors, such as mutational load, appear to be more important in the progression of lymphoma than the off-target effects of antivirals. Studies evaluating the genetic differences between DLBCL patients with resolved HBV and those with current HBV are warranted.
In addition, significant differences were observed in OS between the CHB and non-CHB groups both before and after IPTW. Although antiviral treatment reduces HBV reactivation in CHB patients, the possibility of liver-related death is higher in these patients than in non-CHB patients [47]. Even after antiviral treatment, CHB patients have a greater risk of HCC6 and drug-induced liver injury [48,49] than non-CHB patients, both of which could lead to mortality. Despite these factors, the significantly extended OS in the CHB group compared with the non-CHB group indicates that, in HBV-associated DLBCL, antiviral agents suppress HBV replication and have a synergetic effect with R-CHOP, contributing to prolonged survival.
The present study had several limitations. First, because this was a retrospective study, selection bias may have occurred. However, we conducted a multicenter study and applied multiple statistical methods, including IPTW and multivariable analysis, to overcome this potential bias. Second, the population was restricted to DLBCL patients initially treated with R-CHOP. Patients with HBV-associated DLBCL who underwent chemotherapies other than R-CHOP may experience distinct clinical outcomes. However, by restricting the study population to only these patients, the influence of chemotherapeutic regimens on DLBCL was minimized, focusing on HBV viral load and clinical outcomes.
In conclusion, HBV infection was a favorable prognostic factor associated with a prolonged TTP, PFS, and OS in HBV-related DLBCL patients who received antiviral medication prior to R-CHOP chemotherapy.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement1
Supplement1 Print
Print





