Epidemiology of liver cancer in South Korea
Article information

Abstract
Liver cancer is the sixth most common cancer (fourth in men and sixth in women) and the second largest cause of cancer mortality in South Korea. The crude incidence rate of liver cancer was 31.9/100,000 (47.5/100,000 in men and 16.2/100,000 in women) and the age-standardized incidence rate was 19.9/100,000 (32.4/100,000 in men and 8.8/100,000 in women) in 2014. The crude incidence rate increased from 1999 to 2011 and thereafter showed a subtle decreasing tendency. The crude prevalence rate was 113.6/100,000 (170.2/100,000 in men and 57.1/100,000 in women) and the age-standardized prevalence rate was 72.6/100,000 (115.7/100,000 in men and 33.7/100,000 in women) in 2014, which increased from 2010 to 2014. Survival from liver cancer has improved over the last two decades. The 5-year relative survival rate was markedly increased from 10.7% in those diagnosed with liver cancer between 1993 and 1995 to 32.8% in those diagnosed between 2010 and 2014. The epidemiology of liver cancer is influenced by that of underlying liver diseases such as viral hepatitis. Substantial progress has been made in the prevention and treatment of viral hepatitis; however, uncontrolled alcoholic liver disease, obesity and diabetes appears to have the potential to emerge as major causes for liver cancer. Depending on the success of the control of risk factors, the epidemiology of liver cancer in Korea may change.
INTRODUCTION
Primary liver cancer is the sixth most common cancer and the second largest cause of cancer mortality in the world [1]. The highest incidence rates of liver cancer were observed in Eastern Asia, South-Eastern Asia, Northern Africa and Southern Africa, with China accounting for about 50% of all cases [1]. Approximately 80% of all primary liver cancer is regarded as hepatocellular carcinoma (HCC) [2]. In this review, liver cancer includes all primary liver cancers with disease codes from C22.0 to C22.9 according to the International Classification of Disease codes 10th edition, since reports from GLOBOCAN, Korea Central Cancer Registry and Korea Statistical Information Service are based on those codes. Otherwise, HCC is considered as the disease code C22.0.
INCIDENCE OF LIVER CANCER IN KOREA
In South Korea, a total of 16,178 cases (12,058 cases in men and 4,120 cases in women) of primary liver cancer were diagnosed in 2014, which ranked sixth after thyroid cancer, stomach cancer, colon and rectal cancer, lung cancer and breast cancer (fourth in men and sixth in women) [3]. The crude incidence rate was 31.9/100,000 (47.5/100,000 in men and 16.2/100,000 in women) and the age-standardized incidence rate (adjusted to the Korea standard population using the mid-year population in 2000) was 19.9/100,000 (32.4/100,000 in men and 8.8/100000 in women) [3]. The age-standardized incidence rate adjusted to the world standard population was 19.4/100,000 (31.4/100,000 in men and 8.6/100,000 in women).
In 2000, 13,126 cases of primary liver cancer (9,898 in men and 3,228 in women) occurred. The crude incidence rate was 27.6/100,000 (41.5/100,000 in men and 13.6/100,000 in women) and the age-standardized incidence rate was 27.6/100,000 (46.1/100,000 in men and 12.1/100,000 in women) [3]. The number of cases and crude incidence rate increased to 16,714 cases and 33.4/100,000 (49.3/100,000 in men and 17.4/100,000 in women) in 2011, and showed a subtle decreasing tendency thereafter (Fig. 1). However, the age-standardized incidence rate declined continuously from 28.9/100,000 in 1999 to 19.9/100,000 in 2014 (Fig. 1). The decreasing incidence rates after adjustment appears attributable to population growth (the mid-year population of South Korea changed from 47,534,124 in 2000 to 50,763,158 in 2014) and increasing proportion of older individuals.

Trends in primary liver cancer incidence. Dark grey columns and light grey columns represent the number of male and female incident cases, respectively (left axis). Solid symbols indicate crude incidence rates and hollow symbols indicate age-standardized incidence rates (right axis).
Age- and Sex-specific Incidence
Of 16,178 primary liver cancer cases in 2014, 12,058 were men and 4,120 women with a male-to-female ratio of 2.9:1 [3]. Primary liver cancer was most commonly diagnosed at age 50–59 years (27.3%), followed by 60–69 years (25.2%) and 70–79 years (24.8%). Among women, primary liver cancer was most frequently diagnosed at age 70–79 (32.5%), followed by age 60–69 (23.4%) and age 50–59 (17.3%) years, whereas in men, 30.7% of cases were diagnosed at age 50–59, 25.8% at age 60–69 and 22.2% at age 70–79 years (Fig. 2A). Women were more likely to be diagnosed at older ages compared to men.
Age-specific incidence of liver cancer. (A) Dark grey columns and light grey columns represent the number of male and female incident cases in 2014, respectively (left axis). The black solid line indicates the age-specific incidence rates while the dark grey dashed line and light grey dotted line indicate age-specific incidence rates in males and females, respectively (right axis). (B) Light grey columns and dark grey columns represent the number of cases diagnosed in 2005 and 2014, respectively (left axis). Solid symbols and hollow symbols indicate age-specific incidence rates in 2005 and 2014, respectively (right axis).
Age-specific incidence rates generally declined from 2005 to 2014 over all age groups except for those aged over 80 years (Fig. 2B), even when the number of cases were not decreasing (Fig. 1, 2). When comparing the data from 2005 and 2014, a slight rightshift was observed in the distribution of age at diagnosis (Fig. 2B). Incident cases were most common among those between 50 and 69 years old and were similar for both 2005 and 2014; however, the number of cases diagnosed at age 70 and over increased from 2005 to 2014.
Region-specific Incidence
The incidence of primary liver cancer varied geographically. In 2014, the agestandardized incidence rate was highest in Jeju-do (JJ, 27.4/100,000), followed by Jeollanam-do (JN, 25.7/100,000) and Gyeongsangnam-do (GN, 25.2/100,000) as shown in Fig. 3. A nationwide study indicated higher rates of HBsAg-positivity in Jeju, Jeollanam-do, Gwangju, Busan and Gyeongsangnam-do [4]. Another nationwide survey reported higher rates of anti-hepatitis C virus (HCV) positive tests in Jeollanam-do, Busan, Geyongsangbuk-do and Gyeongsangnam-do [5]. Higher seropositivity might contribute partly to higher incidence of liver cancer; however, other possibilities remain to be elucidated.
Crude and age-standardized incidence of liver cancer by region. Light grey columns and dark grey columns represent crude incidence rates in 2005 and 2014, respectively. Solid symbols and hollow symbols indicate age-standardized incidence rates in 2005 and 2014, respectively. SU, Seoul; BS, Busan; DG, Daegu; IC, Incheon; GJ, Gwangju; DJ, Daejeon; US, Ulsan; SJ, Sejong; GG, Gyeonggi-do; GW, Gangwon-do; CB, Chungcheongbuk-do; CN, Chungcheongnam-do; JB, Jeollabuk-do; JN, Jeollanam-do; GB, Gyeongsangbuk-do; GN, Gyeongsangnam-do; JJ, Jeju-do.
PREVALENCE OF LIVER CANCER IN KOREA
Primary liver cancer was the seventh most prevalent cancer after thyroid cancer, stomach cancer, colon and rectal cancer, breast cancer, lung cancer and prostate cancer (5th in men and 10th in women) in 2014 [3]. There were 57,691 cases (43,192 men and 14,499 women) who had suffered from primary liver cancer in 2014 [3]. The crude prevalence rate was 113.6/100,000 (170.2/100,000 in men and 57.1/100,000 in women) in 2014 [3]. The age-standardized prevalence rate adjusted to the Korean standard population or the world standard population was 72.6/100,000 (115.7/100,000 in men and 33.7/100,000 in women) or 71.8/100,000 (114.2/100,000 in men and 33.5/100,000 in women), respectively [3].
The number of prevalent cases increased from 43,351 in 2010 to 57,691 in 2014 and so had the age-standardized prevalence rate (adjusted to the Korean standard population) from 63.4 in 2010 to 72.6 in 2014 (Fig. 4). The increased prevalence despite decreased incidence of primary liver cancer may be explained by prolonged survival of patients, since prevalence is influenced by both the incidence rate and the average duration of the disease.

Trends in prevalence of primary liver cancer. Dark grey columns and light grey columns represent the number of male and female prevalent cases, respectively (left axis). Solid symbols indicate crude prevalence rates and hollow symbols indicate age-standardized prevalence rates (right axis).
Age- and Sex-specific Prevalence
Of 57,691 primary liver cancer prevalent cases in 2014, 43,192 were men and 14,499 women with a male-to-female ratio of 3.0:1 [3]. Primary liver cancer occurred most commonly between age 60–69 years (32.0%), followed by 50–59 years (29.3%) and 70–79 years (22.8%). Primary liver cancer in female patients was most common in the age group 60–69 years, followed by 70–79 years (29.5%) and 50–59 years (21.7%), whereas primary liver cancer in male patients was most common in the age group 60–69 years (32.4%), followed by 50–59 years (29.3%) and 70–79 (22.8%) years. Female patients tended to be older than male patients were, as shown in incidence trends (Fig. 2A and 5A).
Age-specific prevalence of liver cancer. (A) Dark grey columns and light grey columns represent the number of male and female prevalent cases in 2014, respectively (left axis). The black solid line indicates the age-specific prevalence while the dark grey dashed line and light grey dotted line indicate age-specific prevalence rates of males and females, respectively (right axis). (B) Light grey columns and dark grey columns represent the number of prevalent cases in 2010 and 2014, respectively (left axis). Solid symbols and hollow symbols indicate age-specific prevalence rates in 2010 and 2014, respectively (right axis).
The highest age-specific prevalence rates were observed between 55 and 64 years in both 2010 and 2014 (Fig. 5B). Age-specific prevalence rates increased substantially from 2010 to 2014 in those aged over 55 years.
ETIOLOGY OF HCC IN KOREA
Hepatitis B virus
Hepatitis B virus (HBV) is the predominant etiology of HCC in Korea as well as in China and Taiwan [6]. According to several retrospective studies, HBV accounted for 62~75% of HCC (Table 1) [7-11]. The prevalence rates of HBV infection ranged from 8–10% in the 1980s and early 1990s [12]. As the national immunization program for HBV was implemented in 1995, the prevalence decreased to 2.9% in 2013. According to the Korean National Health and Nutrition Examination Survey in 2014, the age-specific prevalence among those aged 10–19 years and those aged 20–29 years were < 1% and < 2%, respectively, and males aged 30–59 years and females aged 60–69 years had a prevalence of 4–5% and 4%, respectively [12]. Therefore, the prevalence of HBV infection is anticipated to continue to decrease. Taiwanese studies have demonstrated that the HCC incidence rate declined in children who had been immunized at birth compared to non-immunized children from the pre-universal immunization era. Given that liver cancer generally occurs in middle-aged or elderly adults and the national immunization program was implemented in 1995, the decreasing tendency of HBV infection does not appear to have affected the incidence or prevalence of HCC to a larger degree yet.
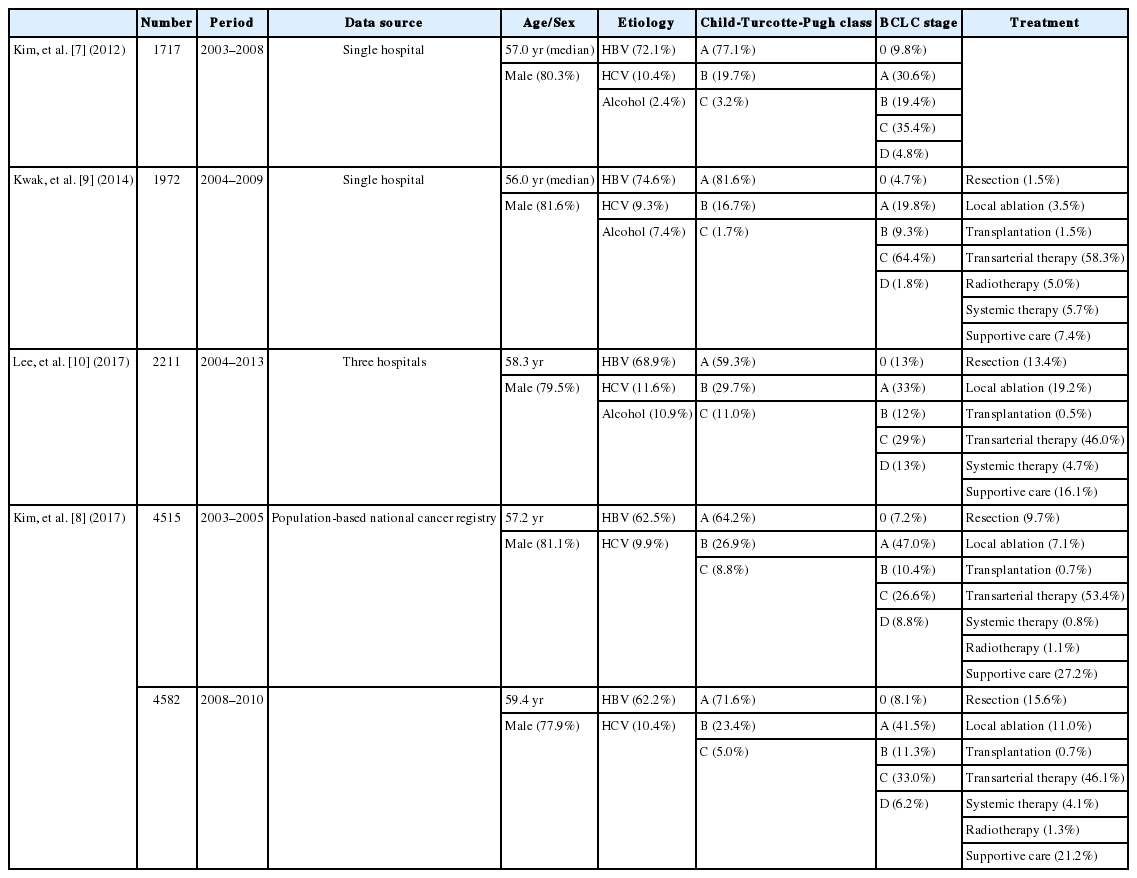
Clinical characteristics of patients diagnosed with hepatocellular carcinoma
Antiviral therapy has been shown to significantly reduce the risk of HCC [13]. Nucleos(t)ide analogues have been introduced with restrictions for financial reimbursement since 1999; however, patients have been able to get a life-long reimbursement since 2010. During that period, the number of patients treated with nucleos(t) ide analogues increased exponentially [14].
Hepatitis C virus
Although HCV is the main cause of HCC in Japan, North America and Europe, it accounts for approximately 10% of HCC cases in Korea [6-11,15]. The prevalence of HCV infection based on anti-HCV positivity was 0.7% in 2014 [16]. No prophylactic vaccine is currently available for HCV; however, the virus can be eliminated by antiviral therapy. New direct-acting antiviral agents have shown excellent outcomes of over 90–95% of sustained virological response [17]. Achieving sustained virological response has been demonstrated to decrease the risk of HCC [18]. In Korea, users of direct-acting antiviral agents have been reimbursed, thus these agents have become utilized to a wider extent since August 2015. Promising results are anticipated; however, the actual influence of antiviral therapy on the incidence of HCC has not been established yet.
Etiologies other than hepatitis virus
Heavy alcohol consumption contributes to the development of HCC, per se , and increases the risk of developing HCC in patients with HBV or HCV infection [19,20]. In Korea, 2.4–10.9% of HCC has been attributed to alcohol use [6,7,9-11]. A prospective observational study reported that 67% of Korean patients newly diagnosed with HCC had a past or current history of alcohol abuse [6]. According to a World Health Organization report on alcohol and health, prevalence of episodic heavy drinking (defined as consumption of at least 60 grams or more of pure alcohol on at least one occasion in the past 30 days) was 12.1% and 0.1% in males and females, respectively, aged 15 years or more [21]. Korean adults above 15 years of age drink an average of 12.3 liters of pure alcohol per year, which translates to 26.7 grams per day [21]. This average consumption remained the same when compared between the years 2008–2010 and the years 2003–2005.
Data are scarce in Korea, however, HCC cases from etiologies other than HBV, HCV, or alcohol ranged from 6.8–15.1% [7,9,11,22]. Nonalcoholic fatty liver disease-associated HCC falls in this category. Nonalcoholic fatty liver disease is considered to be a higher risk factor in North America and Europe than in Asian countries [6]. Since Korea is a HBV-endemic area, prior HBV infection is considered to play a role even in the development of cryptogenic HCC [22]. A recent study reported that 82.1% of patients were positive for anti-HBc in serum and 52.6% were positive for both anti-HBc in serum and HBV DNA in the liver tissue among 78 patients who underwent resection or transplantation for cryptogenic HCC [23].
Diabetes and/or obesity increases the risk of developing HCC and they are closely associated with nonalcoholic fatty liver disease [19]. The prevalence of diabetes and obesity is increasing, and the age-standardized prevalences of diabetes and obesity (body mass index of 25 kg/m2 or higher) in Korean adults were 11.0% and 31.8%, respectively [24]. Recent studies reported that diabetes was found in 21.8–37.1% of Korean patients with cryptogenic HCC [11,23]. It is of concern that nonalcoholic fatty liver disease-associated HCC can also develop in a non-cirrhotic liver [23]. Although a retrospective study showed that the proportion of HCC being based on nonalcoholic fatty liver disease without anti-HBc positivity increased from 3.8% in the years 2001–2005 to 12.2% in the years 2006–2010 [22], further studies are warranted.
NATURAL HISTORY AND MORTALITY OF HCC IN KOREA
According to recent reports on HCC, mean ages were above 55 years and about 80% were male at the time of diagnosis [7-10]. Approximately 60% or more of patients had preserved liver function (Child-Turcotte-Pugh class A). A substantial proportion of patients with HCC are diagnosed at an advanced stage. More than 35% of patients had Barcelona Clinic Liver Cancer C or D stage tumors at the time of diagnosis [7-10]. Transarterial therapies remain the mainstay of treatment modalities [8-10].
The Annual Report of Cancer Statistics has shown the survival gain of primary liver cancer over the last two decades [3]. For those who had been diagnosed with liver cancer between 2010 and 2014, the 5-year relative survival rate was markedly increased from 10.7% to 32.8% compared with those who had been diagnosed between 1993 and 1995 (Fig. 6) [3].
Trends in primary liver cancer survival. Light grey columns and dark grey columns denote 5-year relative survival rates (the ratio of survival rates of individuals who were diagnosed with liver cancer to those who were not) and 10-year relative survival rates, respectively.
A nationwide observational study also demonstrated a significant improvement in overall survival of patients with HCC diagnosed between 2008 and 2010 relative to those diagnosed between 2003 and 2005 even after adjustment for confounding factors [8]. Age-adjusted analysis indicated the improvement of the median survival time from 17.2 months to 28.4 months and 5-year survival rate from 35% to 45%. It is noteworthy that the survival improvement was remarkable in HBV-related HCC, which coincided with the exponential use of oral antiviral agents for HBV [8,9]. Nonetheless, the disease burden of liver cancer does not appear to have decreased yet [14]. A recent study suggested that widespread use of antiviral agents for HBV might increase the number of patients at risk of developing liver cancer as well as the individual’s life expectancy while decreasing the mortality from underlying liver disease [14].
Based on the mortality data from the Korean Statistical Information Service, the crude mortality rate from primary liver cancer was 22.8/100,000 in 2014 (34.0/100,000 in men and 11.6/100,000 in women) and remained stable throughout the last decade (Fig. 7) [25]. Of all cancer mortalities in 2014, it was the second most common cause across all ages following lung cancer, and the most common cause in the fifth and sixth decades of life. The age-standardized mortality rate (adjusted to the mid-year population of 2005 in Korea) was 16.4/100,000 (27.4/100,000 in men and 6.9/100,000 in women) in 2014, decreasing from 22.3/100,000 (37.6/100,000 in men and 9.7/100,000 in women) in 2005 [25]. The discrepancy between crude rate and age-adjusted rate can be observed as with the incidence rate. The age-specific mortality rates increase with age; however, it is of note that a substantial proportion of patients with liver cancer die at a younger age when compared with those with any other type of cancer (Fig. 8).
Trends in liver cancer mortality rates. Dark grey columns and light grey columns represent the number of male and female mortality cases from liver cancer, respectively (left axis). Solid symbols indicate crude mortality rates and hollow symbols indicate age-standardized mortality rates (right axis).
Age distribution of cancer mortality. The upper bar represents percentages of mortality cases from all-sites cancers and the lower bar represents those of mortality cases from liver cancer according to the ages.
CONCLUSIONS
Liver cancer mostly occurs as a complication of underlying liver disease such as viral hepatitis; therefore, the epidemiology of liver cancer is influenced by that of underlying disease. Substantial progress has been made in the prevention and treatment of viral hepatitis and this is expected to affect the epidemiology of liver cancer currently or in the near future. Temporal improvement in overall survival from liver cancer has been demonstrated. However, liver cancer is still the sixth most common cancer and the second largest cause of all cancer mortalities in Korea. Currently, crude incidence rates are stable and prevalence rates are increasing while age-adjusted incidence rates are decreasing. Considering that the disease burden correlates with crude rates of the disease for a given population [26,27]. a careful approach should be taken.
Notes
Authors’ contribution
BH Kim and JW Park were responsible for the acquisition, analysis, and interpretation of the data, and the drafting of the manuscript.
Financial support
This work was supported by the National Cancer Center, Korea (#1510520).
Conflict of Interest
The authors have no conflicts to disclose.
Abbreviations
HBV
hepatitis B virus
HCC
hepatocellular carcinoma
HCV
hepatitis C virus