


Graphical Abstract
INTRODUCTION
An estimated 71 million subjects are infected with hepatitis C virus (HCV) globally. In addition, approximately 400,000 subjects die from chronic hepatitis C (CHC)-related liver cirrhosis and hepatocellular carcinoma (HCC) each year [1]. HCV infection has been rampant in Taiwan with the seroprevalence of anti-HCV antibodies ranging from 3.3% to 8.6% [2,3]. A recent survey in first-time blood donors noted that the age-standardized prevalence of antiHCV antibodies decreased from 27.7 to 9.2 per 1,000 persons in the past two decades, and the age-standardized HCV viremic rate decreased from 5.8 to 3.9 per 1,000 donors between 2013 and 2017 [4]. The World Health Organization has set several goals for controlling viral hepatitis by 2030 [5]. Nevertheless, the majority of countries are currently off track in meeting these goals. The efficacy of the antiviral treatment for CHC is no longer an obstacle for HCV care due to the important invention of direct-acting antivirals (DAAs) [6,7]. Beyond ensuring blood safety and harm reduction, a thorough HCV care cascade involves proper screening of patients who are unaware of their HCV status, accurate and efficient diagnosis, and linking patients to medical care. Each of these steps is a critical hurdle that adds complexity, which prevents the healthcare system from eliminating HCV infection [2,8,9].
To accurately confirm ongoing HCV infection, laboratory testing typically begins with the detection of antibodies to HCV (antiHCV), followed by the confirmation of the presence of HCV RNA in the blood of subjects who are anti-HCV seropositive. The multistep testing procedure represents one of the barriers to HCV care [10]. To ensure the complete and timely diagnosis of HCV, HCV reflex testing is one of the strategies that may simplify the diagnostic algorithms [11]. Namely, the laboratory performs anti-HCV testing first, and if the result is positive, the laboratory will immediately perform an HCV RNA test on the same blood sample. The diagnosis of active HCV infection will be confirmed if the HCV reflex RNA test result is positive, and the individual can then be referred directly for HCV care, which obviates the need for the patient to return for follow-up testing before treatment allocation. Although HCV reflex testing has been consistently applied [12], this strategy has rarely been executed in Taiwan. Moreover, the suboptimal in-hospital referral of viremic patients to liver clinics may also lead to inferior accessibility and poor treatment uptake. We herein made an effort to identify viremic patients by HCV reflex testing and to preemptively transfer them for in-hospital HCV care by using a real-time appointment and late call-back system. To determine the potential improvement due to the scale-up strategies, the treatment gap was compared to that of another antiHCV seropositive patient cohort without the abovementioned intervention in terms of the HCV RNA diagnostic rate and treatment rate.
PATIENTS AND METHODS
Patient enrollment
The order of anti-HCV testing was performed at the clinicians’ discretion depending on the clinical demands. Patients who were newly diagnosed with anti-HCV antibody seropositivity were consecutively enrolled during two time periods in the outpatient departments of a medical center in Taiwan. An in-hospital HCV treatment strategy to scale up the HCV care cascade that included three steps was adopted in December 2019. The first modality involved the use of HCV reflex testing for patients who were antiHCV seropositive. The testing was initiated by the hospital, and all the medical staff were well informed of the policy via email, text and conferences before the strategy was executed.
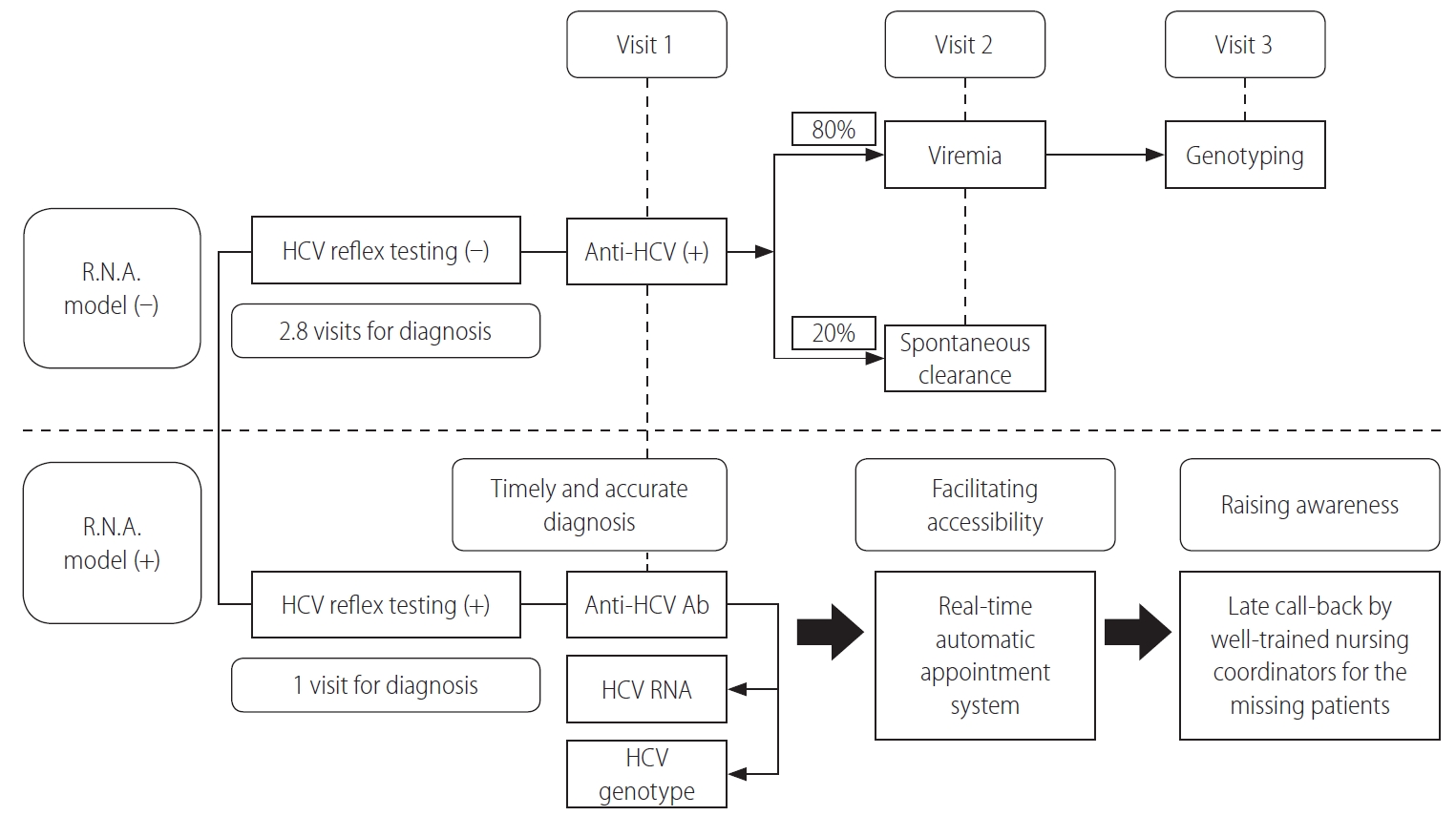
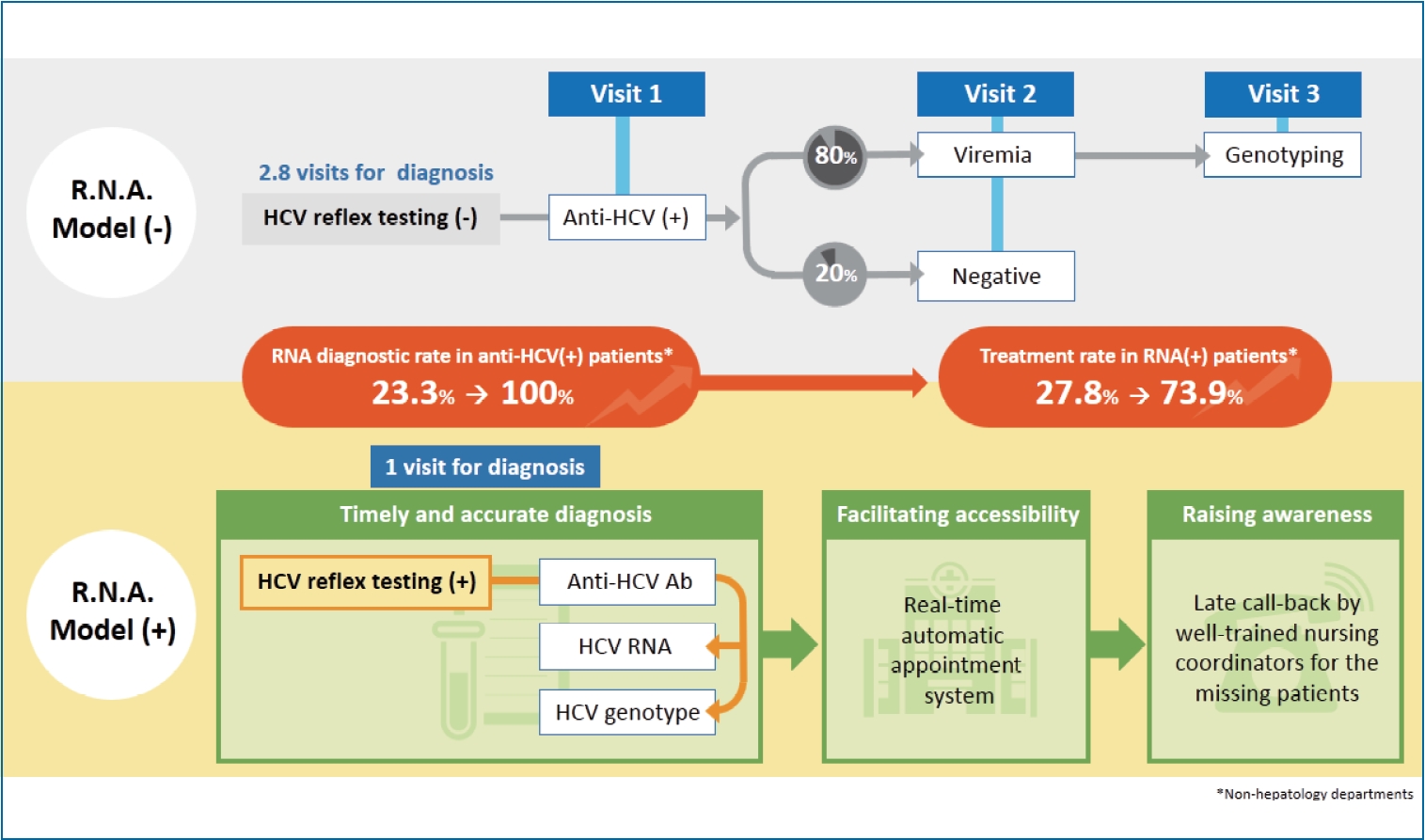
Moreover, an automatic real-time appointment system for the liver clinic was created for patients who were confirmed to have HCV viremia by reflex testing; viremic patients who never visited the liver clinic were referred to the hepatology department immediately for further HCV care regardless of the outpatient department they were visiting at the same time. Finally, a late call back was made by well-trained nursing coordinators for patients from the checklist who missed the appointment (HCV Reflex testing; Call-back by Nursing coordinators; Automatic appointment system, R.N.A. model) (Fig. 1). Subjects who did not receive the R.N.A. strategy were enrolled for comparison between January 2019 and November 2019.
Patients were excluded if they had a history of receiving antiviral therapy, which was clarified by an electronic medical chart review.
DAA treatment
The National Health Insurance Administration of Taiwan began to reimburse DAAs in January 2017, and there are currently no limitations for treating CHC patients with DAAs. The treatment regimens and strategies conformed to the regional consensus [13,14] and regulations of the Health and Welfare Department of Taiwan [15]. The treatment regimens in the current study included sofosbuvir/ledipasvir, sofosbuvir/velpatasvir, elbasvir/grazoprevir, and glecaprevir/pibrentasvir. HCV antibodies were detected by a third-generation enzyme immunoassay (Abbott Laboratories, North Chicago, IL, USA). HCV RNA and the genotypes were determined using a real-time PCR assay (RealTime HCV; Abbott Molecular, Des Plaines IL, USA; detection limit: 12 IU/mL) [16]. The institutional review board of Kaohsiung Medical University Hospital approved the protocols, which followed the guidelines of the International Conference on Harmonization for Good Clinical Practice (IRB approval numbers: KMUHIRB-F(I)-20170053, KMUHIRBE(I)-20200245).
Statistical analyses
Frequencies were compared between groups using the chi-squared test with the Yates correction or Fisher’s exact test. Group means (presented as the mean±standard deviation) were compared using analysis of variance and Student’s t-test or the nonparametric Mann-Whitney test when appropriate. The HCV RNA diagnostic rate and treatment rate were compared between hepatology and non-hepatology departments. All other sections or departments apart from Division of Hepatobiliary Medicine in Kaohsiung Medical University Hospital were categorized as non-hepatology departments. The HCV treatment uptake is defined as the proportion of known viremic patients being treated among all anti-HCV seropositive patients (HCV RNA diagnostic rate multiplied by treatment rate). The statistical analyses were performed using the SPSS ver. 12.0 statistical package (SPSS, Chicago, IL, USA). All statistical analyses were based on two-sided hypothesis tests with a significance level of P<0.05.
RESULTS
After excluding 82 patients with a prior history of antiviral treatment, one hundred and twenty-five patients who adopted the R.N.A. model were recruited up to April 2020. Another 1,396 controls who did not adopt the R.N.A. model were enrolled for comparison. Compared to patients without the intervention, the group that was treated according to the R.N.A. model had a higher proportion of males (59.2% vs. 48.4%, P=0.02). The proportion of patients from non-hepatology departments significantly increased after the implementation of the model (45.6% vs. 18.4%, P<0.001). A higher proportion of patients who received sofosbuvir/velpatasvir was noted in the R.N.A. model group. Other patient characteristics were similar between the two patient cohorts (Table 1). The most common patient source from non-hepatology departments was the Division of Infectious Diseases (n=54), followed by the Department of Otolaryngology (n=53), Department of Psychiatry (n=49), Department of Surgery (n=43), Division of Nephrology (n=31), Division of Endodontics and Operative Dentistry (n=18), Division of Pulmonary Medicine (n=15), Department of Family Medicine (n=13), and others (n=38).
Among anti-HCV seropositive subjects, the HCV RNA testing rate was significantly higher in patients who received reflex testing than in those without reflex testing (100% [125/125] vs. 84.8% [1,184/1,396], P<0.001). Of the patients who received HCV RNA testing, the viremia rate was 80.1% (948/1,184) in the nonreflex testing group and 80.0% (100/125) in the reflex testing group. Among the viremic subjects, the rate of HCV genotyping was similar between patients with or without reflex testing (100% [100/100] vs. 98.9% [938/948], P=0.61). When the patients were stratified according to the referring outpatient department, a significant improvement in the diagnostic rate by RNA reflex testing was particularly noted for patients from non-hepatology departments (100% vs. 23.3%, P<0.001) but not for those from hepatology department (100% vs. 98.7%, P=0.999) (Table 2).
The treatment rate in HCV RNA seropositive patients was 83% (83/100) after the adoption of the R.N.A. model. After excluding two patients who passed away due to liver failure and one patient who decided to receive treatment in a nearby hospital, patients from the hepatology department had a significantly higher treatment rate than those from non-hepatology departments (96.1% vs. 73.9%, P=0.002). Of the 12 patients from non-hepatology departments who did not receive antiviral therapy, eight patients decided to postpone treatment due to fear of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection during hospital visits, three other patients refused treatment due to personal reasons despite being well informed, and the other patient lost contact. The modified treatment rate was 89.5% (34/38) after excluding the eight patients who chose to postpone treatment. Compared to subjects who did not adopt the R.N.A. model, a significant improvement in the treatment rate was observed for patients from non-hepatology departments (73.9% vs. 27.8%, P=0.001) but not for those from hepatology departments (96.1% vs. 97.1%, P=0.66) (Table 2).
Overall, the HCV treatment uptake of known viremic patients among the anti-HCV seropositive patients was similar between patients treated with or without the implementation of R.N.A. model (81.2% vs. 83%, P=0.85). The treatment uptake rate did not differ for the patients from hepatology department (95.8% vs. 96.1%, P=0.76). Instead, the application of the R.N.A. model significantly increased the in-hospital HCV treatment uptake rate from 6.4% to 73.9% for patients from non-hepatology departments (P<0.001) (Table 2).
DISCUSSION
The current study demonstrated that the implementation of HCV reflex testing significantly improved the HCV diagnostic rate. Following an in-hospital automatic transferal system and late callback modality further promoted disease awareness and treatment accessibility. The sequential care cascade particularly worked on patients who originally visited the hospital for reasons other than the treatment of hepatitis. Before adopting the R.N.A. strategy, only one-quarter of the anti-HCV seropositive patients from the non-hepatology departments received HCV RNA testing. Furthermore, only one-quarter of the viremic patients received DAAs, which in turn led to very poor HCV treatment uptake. After launching the strategy, the proportion of patients who came from the non-hepatology departments significantly increased. In addition, a 4-fold improvement in the HCV RNA diagnostic rate after the HCV reflex test and a nearly 3-fold improvement in the treatment rate after automatic transfer was observed, showing drastically scaled up treatment by the in-hospital care cascade. As a result, the huge gap between accurate diagnosis and final treatment was overcome, particularly for patients who originally visited non-hepatology departments.
The accurate and timely diagnosis of HCV infection may pave the way for improved HCV care and is key to facilitating the HCV care cascade. It has been reported that one-third of anti-HCV seropositive patients do not receive HCV RNA testing in developed regions, and the major reason for failing to perform the confirmation test was that the patient did not return for follow-up [10]. Interrupted time series analysis revealed that the implementation of HCV reflex testing had the largest impact on the ability to complete timely HCV RNA testing [17]. Currently, HCV reflex testing has rarely been adopted in Taiwan. Nevertheless, it has been reported that the implementation rate of HCV reflex testing has increased from 31% to 89% among large teaching hospitals in Spain from 2017 to 2019 [12]. The applicability of HCV reflex testing by repeatedly using the same blood sample is based on the high accuracy and degree of correlation compared to those achieved with the use of fresh blood samples [18]. HCV reflex testing is time saving, and it also reduces the cost of transportation and outpatient visit fees before patients from either hepatology or non-hepatology departments receive a confirmation of their infection status. Assuming that the HCV viremia rate is 80% and the HCV spontaneous clearance rate is 20% in anti-HCV seropositive patients, an average of 2.8 visits was needed for patients without reflex testing before they could be allocated to antiviral treatment, while only one visit was needed for patients with reflex testing. The strategy of the RNA model could also be applied to populations at-risk for HCV, such as residents in HCV hyperendemic areas [2,3], prisoners [19], intravenous drug users [20], and patients with uremia under maintenance hemodialysis [21-23], to facilitate HCV microelimination.
Due to the pandemic caused by the SARS-CoV-2 infection, fewer patients have visited the hospital during the past few months after we implemented the R.N.A. strategy. Taiwan successfully controlled the pandemic, and fewer than 450 subjects has been infected with the virus that causes coronavirus disease 2019 (COVID-19) as of June 2020 [24]. Regional guidance has suggested that routine treatment of HCV may not be warranted based on the burden of COVID-19 and local official implementations and regulations [25,26]. It is reasonable that the treatment rate of patients from non-hepatology departments was reduced due to fears of contracting COVID-19. All of these patients originally visited the hospital for reasons other than HCV treatment. Due to the adequate control of the SARS-CoV-2 infection, we took positive action in managing these HCV patients. Because of good compensation, which led to a 100% HCV RNA diagnostic rate, and an aggressive referral strategy, the overall HCV treatment uptake was similar among patients before and after R.N.A. model implementation, even though we faced the critical situation of COVID-19. Notably, nearly half of the patients were referred from non-hepatology departments, and the treatment uptake of those patients was significantly increased, indicating the success of the model in facilitating in-hospital HCV elimination. In conclusion, the implementation of HCV reflex testing followed by active transfer significantly increased HCV treatment uptake. The integration of these strategies allowed for timely and accurate diagnosis by raising disease awareness and facilitating access to liver clinics, which closed the gap between the confirmation of HCV infection and final treatment allocation. This continuous in-hospital care cascade may serve as an exemplar for other primary care systems.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print





