Cardiac diastolic dysfunction predicts poor prognosis in patients with decompensated liver cirrhosis
Article information

Abstract
Background/Aims
Left ventricular diastolic dysfunction (LVDD) is an early manifestation of cardiac dysfunction in patients with liver cirrhosis (LC). However, the effect of LVDD on survival has not been clarified, especially in decompensated LC.
Methods
We prospectively enrolled 70 patients with decompensated LC, including ascites or variceal bleeding, at Daejeon St. Mary’s Hospital from April 2013 to April 2015. The cardiac function of these patients was evaluated using 2D echocardiography with tissue Doppler imaging. The diagnosis of LVDD was based on the American Society of Echocardiography guidelines. The primary endpoint was overall survival.
Results
Forty-four patients (62.9%) had LVDD. During follow-up (22.3 months), 18 patients died (16 with LVDD and 2 without LVDD). The survival rate was significantly lower in patients with LVDD than in those without LVDD (31.1 months vs. 42.6 months, P=0.01). In a multivariate analysis, the Child-Pugh score and LVDD were independent predictors of survival. Moreover, patients with a ratio of early filling velocity to early diastolic mitral annular velocity (E/e’) ≥ 10 (LVDD grade 2) had lower survival than patients with E/e’ ratio < 10.
Conclusions
The presence of LVDD is associated with poor survival in patients with decompensated LC. Therefore, it may be important to monitor and closely follow LVDD patients.
INTRODUCTION
Liver cirrhosis (LC) is one of the most common causes of death worldwide [1]. However, in the early phase of LC, up to 40% of patients are asymptomatic with relatively good prognosis [1]. In decompensated LC, the prognosis worsens with the development of complications [2,3]. In addition to various complications, cardiac function, which is preserved in early LC, decreases with disease progression [2,4].
Recent studies suggest that beta-blockers are only effective within a particular clinical window, i.e., between early cirrhosis and end-stage cirrhosis [2,5]. Outside of this window, beta-blockers may reduce survival in advanced LC due to their negative impact on cardiac reserve [2,5]. Therefore, assessing cardiac function in LC is becoming increasingly important.
Cardiac dysfunction in cirrhotic patients, known as cirrhotic cardiomyopathy, is characterized by the following three factors: impaired contractile responsiveness to stress, diastolic dysfunction, and electrophysiological abnormalities with a prolonged QT interval [6,7]. The key pathogenic mechanisms underlying cirrhotic cardiomyopathy include impairment of β-receptor signaling, membrane fluidity, and overactivity of endogenous substances such as nitric oxide [7,8].
Among the three factors that contribute to cirrhotic cardiomyopathy, left ventricular diastolic dysfunction (LVDD) is known to be an early marker of cardiac dysfunction in LC patients [9]. The rate of LVDD is higher in decompensated LC versus compensated LC [10]. However, it is difficult to diagnose LVDD using Child-Pugh scores or electrocardiogram (ECG). Indeed, LVDD can only be diagnosed using echocardiography [7]. Moreover, the prognosis of patients with LVDD in decompensated LC has not been well investigated. According to the “window hypothesis”, cardiac reserves decrease as the disease progresses and mortality increases correspondingly [2,5]. Thus, we hypothesized that patients with LVDD have poor prognosis compared to those without LVDD among patients with decompensated LC. In this study, the incidence and survival rate of decompensated LC patients with LVDD were evaluated.
MATERIALS AND METHODS
Study population
A total of 70 patients with decompensated LC, including ascites or variceal bleeding, were prospectively enrolled at Daejeon St. Mary’s Hospital from April 2013 to April 2015. LC was diagnosed based on laboratory findings and imaging studies and/or histologic findings. Decompensation in cirrhotic patients was defined as a Child-Pugh score ≥ 7 and/or the presence of ascites, variceal bleeding, or hepatic encephalopathy. Exclusion criteria included: (1) underlying heart, lung, or kidney disease; (2) diagnosed hepatocellular carcinoma (HCC); (3) other malignancy; (4) uncontrolled diabetes mellitus; and (5) uncontrolled hypertension. All enrolled patients provided informed consent concerning the collection of their medical data. This study was approved by the institutional ethics review board of Daejeon St. Mary’s Hospital (DC14OISI0072) and complied with the Declaration of Helsinki.
Clinical and laboratory data
Detailed medical history and demographic data were recorded at the time of admission or during outpatient clinic visits. All patients underwent laboratory examinations including a complete blood count and measurement of biochemical parameters, coagulation profiles, and pro-brain natriuretic peptide (pro-BNP) and high-sensitivity C-reactive protein (hs-CRP) levels. Child-Pugh and Model for End-stage Liver Disease (MELD) scores were calculated using laboratory findings. The hepatic venous pressure gradient (HVPG) was also obtained by measuring wedged and free hepatic venous pressure.
Electrocardiography and echocardiography
All patients underwent ECG (Pagewriter Trim III; Philips, Amsterdam, Netherlands) and the corrected QT interval (QTc) was calculated using Bazett’s formula. Two-dimensional echocardiography with tissue Doppler imaging (TDI) (Vivid E9; General Electric, Boston, MA, USA) was performed by an experienced operator, and all procedures were conducted in accordance with the recommendations of the American Society of Echocardiography (ASE) [11]. The following parameters were measured using M-mode, a pulsed-wave Doppler, and TDI: heart rate, left ventricular ejection fraction (LVEF %) using the modified Simpson’s rule, left atrium volume index (LAVI), isovolumetric relaxation time (IVRT), peak early filling velocity (E), atrial filling velocity (A), calculated E/A ratio (E/A), deceleration time of the E wave (DT), average early diastolic mitral annular velocity of the septal and lateral sites (e’), and calculated E/e’ ratio (E/e’).
LVDD was defined and classified according to the recommendations of the ASE [11], as follows: grade 1 LVDD: e’ <8 cm/sec, E/A ratio <0.8, E/e’ ratio <9, and DT >200 ms; grade 2 LVDD: e’ <8 cm/sec, E/A ratio 0.8–1.5, E/e’ ratio 9–15, and DT 160–200 ms; and grade 3 LVDD: e’ <8 cm/sec, E/A ratio >2, E/e’ ratio >15, and DT <160 ms.
Statistical analysis
Patient characteristics are presented as means ± standard deviation (SD) or as counts, as appropriate. Student’s t test or the Mann-Whitney tests were used to compare continuous variables. For evaluating categorical data, the chi-square test with Fisher’s exact test was used. Survival curves were estimated using Kaplan-Meier’s analysis. The Cox proportional hazards model was used to evaluate the predictive factors for survival. Variables with a P-value<0.2 in the univariate model were re-evaluated using a multivariate Cox’s proportional hazard model. All statistical analyses were performed using SPSS software (ver. 15.0; IBM Corp., Armonk, NY, USA).
RESULTS
Clinical baseline characteristics
Eighty-four patients with decompensated LC were screened in this cohort study. Of these, 70 patients were included and 14 were excluded due to fulfilment of the following criteria: underlying HCC (n=10), other underlying malignancy (n=2; renal cell carcinoma, cholangiocarcinoma) or underlying heart disease (n=2; atrial fibrillation, dilated cardiomyopathy) (Fig. 1).

Study flow chart of patients included in the study. LC, liver cirrhosis; HCC, hepatocellular carcinoma.
The baseline characteristics of the patients are listed in Table 1. Of the 70 included patients, 44 had LVDD and 26 did not have LVDD. Of the LVDD patients, 34 had grade 1 LVDD and 10 had grade 2 LVDD. The mean age of participants was 54.3±10.5 years and the mean age of the LVDD group was higher than that of the normal group (P<0.001). The majority of patients were male (78.6%), and alcohol was the main etiology for both groups (normal, n=17; LVDD, n=30). Of all patients, 18 (25.7%) belonged to Child-Pugh class A, 35 (50.0%) belonged to class B, and 17 (24.3%) belonged to class C. The percentage of patients in each Child-Pugh class did not differ between the normal and LVDD groups (P=0.725). Moreover, there were no significant differences between the two groups in MELD score, pro-BNP level, HVPG, or DT. However, the LVDD group had significantly prolonged QTc values (P<0.001), higher E/e’ ratios (P<0.001), and lower E/A ratios than participants without LVDD (P<0.001).

Comparison of baseline characteristics between patients with and without diastolic dysfunction
Overall survival
The median follow-up period was 22.3 months (range: 0.2–45.6 months). During follow-up, 18 patients (25.7%) expired. All 18 patients died due to LC complications: hepatorenal syndrome (n=6), hepatic failure (n=5), sepsis (n=4), and variceal bleeding (n=3). Of these patients, 16 were in the LVDD group (16/44, 36.3%) and 2 (2/26, 7.7%) were in the normal group. In a Kaplan-Meier survival analysis, the LVDD group showed significantly lower survival than the normal group (31.1±2.8 months vs. 42.6±1.8 months, P=0.01; Fig. 2).
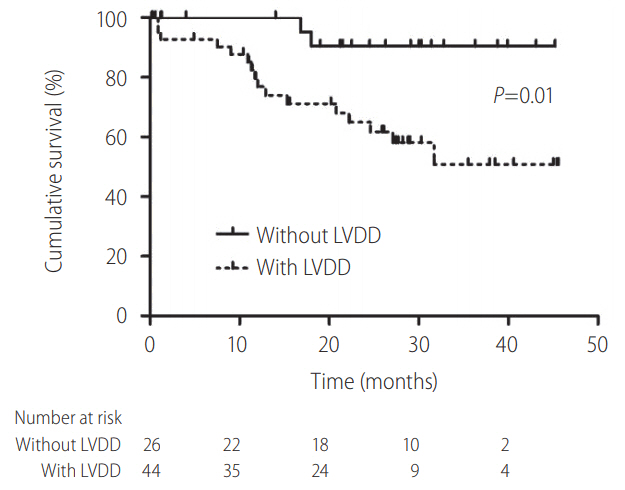
Kaplan-Meier survival curve of patients with and without diastolic dysfunction. In decompensated cirrhosis, patient with left ventricular diastolic dysfunction (LVDD) had lower survival than patients without LVDD (P=0.01).
Predictive factors for overall survival
Table 2 shows the predictive factors for survival in patients with decompensated LC. In a univariate analysis, the factors with P-values<0.20 were age, sex, hs-CRP, Child-Pugh score, MELD score, LVEF, QTc, and the presence of LVDD. In a multivariate analysis, the presence of LVDD was an independent predictor of survival in patients with decompensated LC (hazard ratio [HR], 4.69; 95% confidence interval [CI], 1.06–20.8; P=0.042). Additionally, the Child-Pugh score was also a predictor of survival in a multivariate analysis (HR, 1.37; 95% CI, 1.11–1.70; P=0.004).

Cox-regression model for predicting survival
LVDD grade and E/e’ ratio affect overall survival
The overall survival rate was evaluated according to the LVDD grade (Fig. 3). All LVDD groups had significantly lower survival than the normal group regardless of LVDD grade (grade 1 LVDD vs. normal, P=0.03; grade 2 LVDD vs. normal, P<0.01). Although there was no statistically significant difference in survival rate between patients with grades 1 and 2 LVDD (P=0.13), there was a trend toward patients with grade 2 LVDD having lower survival (21.7±5.3 months vs. 32.9±3.1 months).
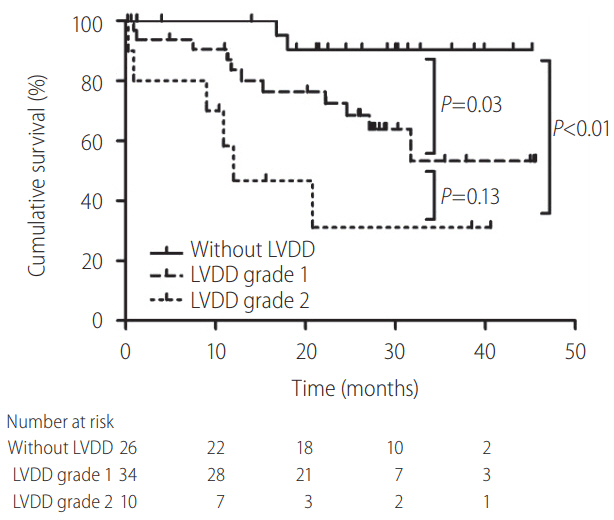
Kaplan-Meier survival curve according to grade of diastolic dysfunction. All left ventricular diastolic dysfunction (LVDD) groups had lower survival than the normal group (grade 1 LVDD vs. normal, P=0.03; grade 2 LVDD vs. normal, P<0.01). In the LVDD group, patients with grade 2 LVDD had lower survival than patients with grade 1 LVDD, without statistical significance (P=0.13).
In addition, to determine useful markers of diastolic dysfunction, patients were classified based on E/e’ ratio values (cut-off value: 10) according to the recently updated guideline [12]. Patients with an E/e’ ratio ≥10 had lower survival than patients with an E/e’ ratio <10 (28.0±2.3 months vs. 37.0±4.6 months, P=0.048, Fig. 4).
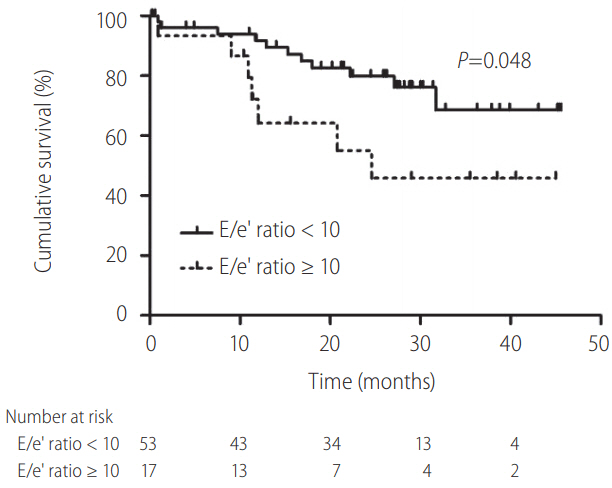
Kaplan-Meier survival curve according to E/e’ ratio. Patients with E/e’ ratio ≥10 had lower survival than patients with E/e’ ratio <10 (P=0.048). E/e’ ratio, ratio of early diastolic annular velocity to peak early diastolic annular wave velocity.
DISCUSSION
In this study, the prevalence and survival rate of LVDD in decompensated LC patients were examined. A total of 70 decompensated LC patients were included, among whom 44 had LVDD. LVDD was significantly associated with poor survival in decompensated LC patients, and LVDD was an independent predictor of survival. Moreover, an E/e’ ratio value ≥10 was a marker of poor survival in our study.
The prevalence of LVDD in our study (44/70, 62.9%) was higher than the previously reported rate of 50% in cirrhotic patients [13]. Cardiac and circulatory dysfunction may be more severe in decompensated LC [7], which may have resulted in the higher rate of LVDD seen in our study. Similar to previous studies demonstrating that LVDD precedes systolic dysfunction [9,14], systolic function in both the LVDD and normal groups was well preserved in this study. However, because E/e’ ratio and E/A ratio are one of factors to evaluate LVDD [11,12], E/e’ ratio and E/A ratio were different between the two groups. Moreover, prolonged QTc, which is one of findings in cirrhotic cardiomyopathy [7,14], was noted in LVDD group.
As Child-Pugh score is already a well-known predictor for survival in LC [15,16], Child-Pugh score was one of the predictive factors for survival in multivariate Cox-regression model of this study. On the other hand, hs-CRP, QTc, pro-BNP were not a predictive factor for survival in our study. In prior studies, similarly with our study, hs-CRP was not documented as a predictor for survival or only high-level of CRP (>32 mg/L) was associated with mortality [17,18]. Although some studies suggested that QTc prolongation was associated with poor prognosis [19,20], there was no survival difference after adjusting Child-Pugh score in LC patients [20,21]. In some studies, pro-BNP was also supposed to be associated with survival in LC patients [22-24]. However, when evaluating with LVDD, pro-BNP has no significance for survival in accordance with our study [16].
Our most important finding concerns the prognostic value of LVDD for survival. In this study, patients with LVDD had significantly lower survival than those without LVDD (P=0.048). In a multivariate Cox regression model, the presence of LVDD was also an independent predictor of survival (P=0.042). Moreover, the presence of LVDD had a significantly higher HR than the Child-Pugh score, which was the other predictor of survival in this study (HR 4.69 vs. 1.37). The clinical relevance of these results is significant considering the asymptomatic nature of LVDD in cirrhotic patients, with ascites or variceal bleeding masking cardiac reserve impairment. Thus, early diagnosis of LVDD is necessary for the appropriate management of decompensated cirrhotic patients.
The ideal treatment for LVDD would be pharmacological agents that facilitate myocardial relaxation and improve LV compliance. However, treatment of LVDD remains largely empiric in clinical practice because there have been no randomized trials evaluating the effects of therapeutic agents. Practically, reducing overloading conditions (preload and afterload) and controlling heart rate are the therapeutic goals of LVDD [25]. Angiotensin converting-enzyme inhibitors, angiotensin II receptor blockers, and beta blockers have been used to attain this goal [25]. Additionally, in grade 2 LVDD patients, adding diuretics including aldosterone antagonists may prove useful [25]. However, in end-stage cirrhosis, these medical therapies may negatively impact cardiac reserve and survival according to window theory [2]. Further studies are warranted to investigate potential useful pharmacological agents based on LVDD status, including beta blockers. Liver transplantation (LT) could be also an alternative option for these end-stage liver disease patients. Therefore, according to the status of liver function and cardiac reserve, proper medical therapies or LT may be needed in decompensated LC patients with LVDD.
All LVDD groups had significantly lower survival than patients without LVDD. Moreover, grade 2 LVDD patients had lower survival than grade 1 LVDD patients, although this difference was not statistically significant (P=0.13). Ruíz-del-Árbol et al. previously demonstrated that patients with grade 2 LVDD had lower survival than grade 1 LVDD patients [26] in a study that included a similar number of grade 1 (n=19) and grade 2 (n=18) cases. However, our study included fewer grade 2 patients (n=10) compared to those with grade 1 LVDD (n=34). Moreover, as our patients included only those with decompensated LC, even the grade 1 LVDD patients had a lower survival rate than those of the prior study. These factors could have contributed to the statistically negative results of our study. It may be yield similar results to previous data if we include greater number of grade 2 LVDD patients [26].
The E/e’ ratio is an important marker for diagnosing and grading LVDD [11,12]. According to recent guidelines, higher E/e’ ratios (≥10) are associated with severe LVDD, i.e., of grade 2 or 3 [12]. Moreover, in our study, a higher E/e’ ratio (≥10) was associated with significantly lower survival rates and a lower E/e’ ratio (<10). Thus, the E/e’ ratio may be a useful prognostic marker to determine severe LVDD and poor survival in patients with decompensated LC.
Our study had several limitations. First, it included patients from only a single center. Moreover, only a small number of patients (n=70) were included. However, the prospective design and relatively long follow-up period were strengths of this study. Moreover, this study included real clinical practice data of decompensated LC patients among a group of homogeneous Korean individuals. We were unable to clearly explain the relationship between LVDD and the lower survival rate in our decompensated LC patients. Because cirrhotic cardiomyopathy contributes to various complications in LC, the presence of LVDD, which represents the earliest sign of cirrhotic cardiomyopathy, seems to result in a lower survival rate. Further studies are required to demonstrate the pathogenic relationship between LVDD and the prognosis of patients with decompensated LC.
In conclusion, we here demonstrate that LVDD is associated with poor survival in patients with decompensated LC. Moreover, an E/e’ ratio ≥10 is associated with higher mortality. Therefore, the presence of LVDD and the E/e’ ratio value must be determined in patients with decompensated LC. Early treatment including medical therapy and LT should be considered in patients with LVDD.
Notes
Author contributions
Lee SK analyzed data and wrote the paper; Kim SH and Ahn HJ collected the data; Song MJ designed the study and analyzed the data.
Conflict of Interest
The authors have no conflicts of interest to disclose.
Abbreviations
A
arterial filling velocity
ASE
American Society of Echocardiography
DT
deceleration time of E wave
E
peak early filling velocity
e’
average of septal and lateral site of early diastolic mitral annular velocity
E/A
calculated E/A ratio
ECG
electrocardiography
E/e’
calculated E/e’ ratio
HCC
hepatocellular carcinoma
hs-CRP
high-sensitivity C-reactive protein
HVPG
hepatic venous pressure gradient
IVRT
isovolumetric relaxation time
LAVI
left atrium volume index
LC
liver cirrhosis
LT
liver transplantation
LVDD
left ventricular diastolic dysfunction
LVEF
left ventricle ejection fraction
MELD
Model for End-stage Liver Disease
pro-BNP
pro-brain natriuretic peptide
QTc
corrected QT interval in ECG
TDI
tissue Doppler imaging
WHVP
wedged hepatic venous pressure
References
Article information Continued
Notes
Study Highlights
Due to uncertainty of the effect of left ventricular diastolic dysfunction (LVDD) in decompensated liver cirrhosis (LC), we evaluated the effect of LVDD in decompensated LC on survival. Of 70 enrolled patients, 18 died during follow-up (22.3 months). The survival rate was significantly lower in patients with LVDD than in those without LVDD (31.1 months vs. 42.6 months, P=0.01). In a multivariate analysis, the Child-Pugh score and LVDD were independent predictors of survival. Therefore, the presence of LVDD is associated with poor survival in patients with decompensated LC.