

INTRODUCTION
Chronic hepatitis C affects an estimated 1-2% of the Korean population and is one of the leading causes of liver cirrhosis and hepatocellular carcinoma in Korea.1 Over the past decade, pegylated interferon (peginterferon) and ribavirin combination therapy has become the standard antiviral treatment for chronic hepatitis C regardless of hepatitis C virus (HCV) genotype. Although standard peginterferon and ribavirin combination therapy achieves better response rates than previous interferon and ribavirin combination therapy or peginterferon monotherapy, a high proportion of patients still suffer from treatment failure or adverse effects of the therapy.
The recent results of clinical trials show that there has been much progress in the treatment of chronic hepatitis C. Viral kinetics during antiviral treatment has emerged as an important predictor of treatment response and is used to guide treatment: the more rapidly HCV RNA disappears during treatment, the higher the response rate to treatment is. This suggested that the viral response to treatment could be used to modify treatment duration. Response-guided therapy, the concept of 'customized therapy depending on viral response', which modifies the treatment period depending on the viral response, is a newly emerging 'proof of concept'. Shorter treatments would not only improve overall tolerability, but also reduce unnecessary medication and expense.
In this article, we reviewed recently updated American Association for the Study of Liver Disease (AASLD) and European Association for the Study of the Liver (EASL) practice guidelines for chronic hepatitis C,2-4 and compared them with Korean data. Upcoming DAAs were also mentioned. We focused on the factors affecting treatment, response guided treatment, retreatment after failure of standard treatment, management of adverse events during treatment, and new treatment options.
Factors affecting the duration and outcome of treatment for chronic hepatitis C
With the development of peginterferon, treatment outcomes have improved and combination therapy with peginterferon and ribavirin is currently acknowledged to be the standard antiviral treatment of chronic hepatitis C.
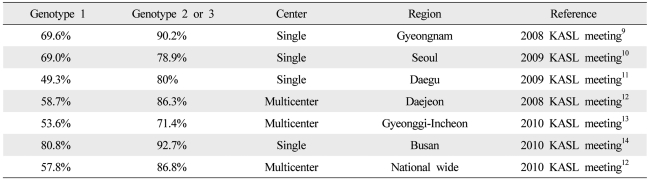
The viral genotype is one of the most important factors affecting the duration and outcome of antiviral treatment.2 Among the six genotypes of HCV, 48 week combination therapy is recommended as standard treatment for genotypes 1 and 4, whereas 24 week combination therapy is recommended for genotypes 2 and 3.1 Further studies are needed to define the standard duration for genotype 6, the most common genotype in Asia. In Western countries, the reported sustained virological response (SVR) rate is 40-50% for genotype 1 and 70-80% for genotypes 2 and 3.5 A higher response rate is reported in Korea: the SVR rate of genotype 1 is around 60-70% and those of genotypes 2 and 3 reach 80-90% (Table 1). However more prospective studies are needed in Korea because most of the studies have been retrospective and there are many differences in treatment outcomes by research institutes.
A low baseline HCV RNA level before treatment as well as the viral genotype is important factors affecting treatment outcome, and has considerable influence on decisions about duration of treatment in patients showing rapid virological responses. A low HCV RNA level is defined as <600,000 IU/mL by AASLD and 400,000-800,000 IU/mL by EASL.4
A host genetic polymorphism upstream of the IL28B gene on chromosome 19 has been recently identified as a strong indicator of a SVR to combination therapy with peginterferon alpha and ribavirin and spontaneous clearance of acute HCV infection, particularly in asymptomatic patients.6,7 The IL-28B polymorphism can help explain individual and racial differences in responses to standard combination therapy. However, additional studies are needed because IL-28B as a predictor has some disadvantages such as low accuracy in predicting treatment success in individual patients.
Other factors affecting the outcome of treatment include the stage of fibrosis, body mass index, insulin resistance, age, gender, and co-infection with another hepatotropic virus or with HIV.8
Viral kinetics in chronic hepatitis C
Undetectable HCV RNA in a sensitive assay at treatment week 4 is referred to as rapid virological response (RVR).4 A sensitive HCV RNA assay is defined as one with a lower limit of detection of 50 IU/mL.4 It is known that the probability of a SVR is high regardless of viral genotype when RVR is attained. Although early termination of antiviral therapy may be considered in some selected patients with RVR, absence of RVR does not justify extending the duration of treatment because of its low predictability.15-18
An early virological response (EVR) is defined as a 2 log reduction of HCV RNA levels or the disappearance of HCV RNA at treatment week 12. A partial EVR (pEVR) is defined as detectable but at least 2 log decrease in HCV RNA levels compared to baseline level, and a complete EVR (cEVR) is defined as undetectable HCV RNA at treatment week 12.2 A virological response at treatment week 12 is known as a predictor of SVR in genotype 1 chronic hepatitis C.19,20
The AASLD practice guidelines recommend that treatment should be stopped if HCV RNA is detectable at treatment week 24 and extended to 72 weeks if HCV RNA is negative at treatment week 24 in genotype 1 patients with pEVR. However, the EASL practice guidelines recommend that the HCV RNA level should be measured at treatment week 4 and 12 regardless of genotype and treatment be stopped in genotypes 2 and 3 as well as 1 if there is not at least a 2 log decrease of HCV RNA from baseline.4
Short term therapy in patients with rapid virological response
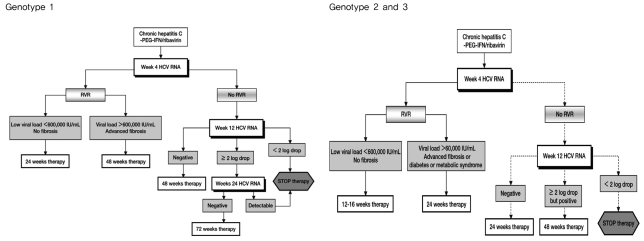
In genotype 1 chronic hepatitis C, it is reported that the treatment outcomes of 24 week short term therapy are comparable to those of 48 week standard therapy in patients with RVR and low pre-treatment HCV RNA levels (<600,000 IU/mL).16,21-23 There have been two studies of short term therapy in genotype 1 patients in Korea. One study of 50 patients with RVR reported that the number of SVR with 24 week short term therapy did not differ from that with 48 week therapy.24 The other retrospective study of 343 patients reported that all patients with low HCV RNA levels before treatment and RVR after treatment attained SVR with 24 week short term therapy.14 The recent EASL practice guidelines recommend 24 week therapy for patients who have low pre-treatment HCV RNA levels (400,000-800,000 IU/mL) and attain RVR.4 Short term therapy can be considered selectively in genotype 1 patients with low baseline HCV RNA levels who achieve RVR when maintaining the therapy is difficult because of adverse effects (Fig. 1). However, additional prospective randomized control studies are needed in Korea.
In recent studies with genotype 2 and 3 chronic hepatitis C, shortening of treatment from 24 to 16 weeks resulted in the same treatment outcomes in terms of SVR in patients who attained RVR.2,17,18 In addition, a retrospective Korean study of 163 chronic hepatitis C patients found no difference in SVR between 16 week short term therapy and 24 week standard therapy (96.8% vs. 95.1%) in patients with genotype 2 or 3 who had reached RVR.14 EASL practice guidelines recommend short term therapy of 12-16 weeks be considered in patients with RVR and low baseline viral loads (<400,000-800,000 IU/mL), but the evidence for the equal efficacy of shortened treatment is insufficient in patients with negative predictors of response such as advanced fibrosis and cirrhosis, metabolic syndrome, insulin resistance, and hepatic steatosis.4 In summary, short term therapy can be considered selectively in genotype 2 and 3 patients if they have RVR, low baseline viral loads, and no negative response predictors (Fig. 1).
Extended therapy in patients with delayed viral response
A delayed viral response (DVR) is defined as undetectable HCV RNA at treatment week 24 in genotype 1 patients with pEVR. In recent studies, 72 week extended therapy yielded significantly more SVR than 48 week standard therapy in genotype 1 patients with DVR.25,26 In Europe, 72 week extended therapy is recommended for genotype 1 patients showing DVR (Fig. 1).4 Another study obtained the opposite result27 and there are no data in Korea yet. Therefore, extended therapy for genotype 1 patients should be used with care, taking into account the patients' characteristics before treatment, adverse effects of treatment, compliance and socio-economic circumstances of the patients as well as virological responses to treatment.
EASL practice guidelines recommend 48 week extended therapy for genotype 2 and 3 patients with pEVR (Fig. 1).4 However, study results for extended therapy for genotypes 2 and 3 are very limited and domestic data are insufficient. For genotype 4 patients, therapy as for genotype 1 is recommended, but there are no recommendations for 'response guide treatment' relating to genotypes 5 and 6.
Retreatment of patients who failed standard therapy
A quarter of patients who receive standard therapy with peginterferon and ribavirin experience treatment failure and do not attain SVR. Treatment failure can be divided into non-response and relapse. Studies of retreatment with peginterferon and ribavirin have reported that SVR rate was 42% in the relapsed patients who had treated with non-pegylated interferon and ribavirin,28 and 33% in the relapsed patients who had treated with peginterferon and ribavirin.29 There have been two large retreatment clinical trials on non-responders after 48 week standard treatment (EPIC-3, REPEAT). The SVR rates after retreatment was as low as 6% in the EPIC-3 program and 9% in the REPEAT trial. However, the SVR rates did increase significantly but only to 16% when 72 week extended treatment was performed in the REPEAT trial.30 Interestingly, treatment success rates were relatively high in both the EPIC-3 and REPEAT trials when EVR was obtained after retreatment.
Two retrospective studies regarding the retreatment of Korean patients have been published as abstracts. The results in summary are as follows. Among patients who had used peginterferon and ribavirin, SVR rate was 0% (n=1) in the non-responders and 70% (n=10) in the relapsed patients. Among patients who had used non-pegylated interferon and ribavirin, SVR rate was 17.6% (n=17) in non-responders and 81.3% (n=16) in relapsed patients.31,32
In conclusion, retreatment with peginterferon and ribavirin should be considered in patients who received non-pegylated interferon or peginterferon monotherapy.2 However, when SVR is not attained despite an adequate period of treatment with peginterferon and ribavirin, careful consideration should precede retreatment with the same drugs. In Europe, retreatment is not recommended for non-responders to standard therapy that includes peginterferon. In such cases, triple combination therapy including a protease inhibitor which is expected to be released onto the market soon may be considered.
Management of adverse effects during treatment
Adverse effects associated with combination therapy with interferon and ribavirin are relatively frequent. It has been reported that 10-14% of patients discontinued treatment because of adverse effects.20,33
A decrease in hemoglobin develops within the first 4 weeks after initiation of the therapy and larger doses of ribavirin result in more severe decrease. Ribavirin is contraindicated in the patients with chronic renal failure because the risk of hemolytic anemia is high by the accumulation of ribavirin. It is currently recommended to reduce the ribavirin dose to 600 mg if Hb decreases to <10 g/dL and to discontinue ribavirin if Hb is <8.5 g/dL. However, as SVR is higher in patients treated with high dose ribavirin in the initial phase and decreases dramatically when the dose is reduced within the first 12 weeks of treatment, careful consideration is needed before making a decision to reduce the ribavirin dose in asymptomatic anemic patients. Although with a lack of evidence about whether the use of erythropoietin (EPO) increases treatment success, the use of EPO in the initial phase of treatment (within the first 12 weeks) may decrease the frequency of ribavirin dose reduction, and improve the general condition of patients, and thus increase the drug compliance and the SVR. Therefore, selective use of EPO should be considered if hemoglobin is <10 g/dL.
Neutropenia is defined as <1,500 neutrophils/mm3 (ANC) and severe neutropenia is defined as ANC <500/mm3 in peripheral blood. Both occur in 18-20% and 4% of the patients during treatment respectively. It was recommended in a large study to halve the dose of peginterferon if ANC is reduced to <750/mm3 and to discontinue peginterferon if ANC is reduced to <500/mm3. However, no accurate clinical guidance regarding neutropenia has been established.20,33,34 Granulocyte colony stimulating factor (G-CSF) is often used in severe neutropenic patients with fever after anti-cancer therapy, and has been shown to reduce mortality associated with infections. While a number of clinicians have tried using G-CSF in the antiviral therapy of chronic hepatitis C, cases other than hepatic cirrhosis patients requiring G-CSF are rare as severe infections are not common during the therapy even in cases of neutropenia.35 In the studies that used 150-300 µg of G-CSF weekly, increase in ANC, not in SVR was demonstrated.36,37
As for platelets, it is recommended to halve the dose of peginterferon if they decline to <50,000/mm3 and to discontinue peginterferon if they are <30,000/mm3. In a phase II clinical trial, eltrombopag, an oral thrombopoietin mimetic, was shown to increase platelet count in type C hepatic cirrhosis patients and significantly increased the number of patients who were able to complete 12 week antiviral treatment.38 A phase III clinical trial is required to evaluate its effects on SVR.
New hepatitis C drugs
The most studied DAAs against hepatitis C virus are telaprevir (TVR) and boceprevir (BOC), which are NS3/4 protease inhibitor.
Although TVR induced rapid and extensive virus inhibition in 14 day monotherapy in phase I clinical trial (a 4.4 log reduction from that before treatment) and awakened great expectations, virological breakthrough due to the emergence of drug-resistant strains occurred in a number of patients who received it as monotherapy. Therefore trials to improve SVR by combining TVR with peginterferon and ribavirin have been undertaken. In the PROVE1 and PROVE2 trials, a marked increase of SVR was observed when this combination was used for the initial 12 weeks in treatment-naive genotype 1 patients (60-69% vs. 48%), and in the PROVE3 study, a notable increase of SVR was seen when the same treatment was used in treatment-experienced genotype 1 patients (51-53% vs. 14%).39-41
BOC, a reversible covalent inhibitor of the NS3/4 protease similar to telaprevir, had a strong antiviral effect in vitro, and was effective when combined with peginterferon. In patients with genotype 1 hepatitis C who had not responded to the initial therapies in phase I clinical trial, the combination of BOC with peginterferon decreased HCV RNA more effectively than monotherapy with BOC or peginterferon.42,43 Recently, the results of the comparison of triple therapy (BOC plus standard therapy) with standard therapy in 1097 patients with genotype 1 chronic hepatitis C have been reported (SPLINT-2 study).42 In that trial, SVR rate for the 24 week and 44 week treatment groups receiving the boceprevir-containing regimen were 66% and 67%, respectively, which were significantly higher than the 40% in the standard therapy. The addition of BOC to peginterferon-ribavirin also resulted in significantly higher SVR rate than that of peginterferon-ribavirin alone in previously treated genotype 1 chronic hepatitis C patients (66% vs. 21%, respectively).
The use of BOC or TVR in combination with peginterferon alfa and ribavirin is accepted as the optimal therapy for genotype 1 in recently updated AASLD guideline.3 Triple therapy involving the addition of a protease inhibitor or other DAAs to the present standard therapy could soon become the standard treatment. In particular, a role for protease inhibitors may be anticipated in the retreatment of patients in whom peginterferon and ribavirin combination therapy have failed.
CONCLUSION
The goal of antiviral treatment in chronic hepatitis C is eradication of HCV to prevent progression of the liver disease. Antiviral therapy based on peginterferon and ribavirin combination therapy achieves an acceptable response rate, and response guided therapy improves response rate and tolerability by reducing medication and expense. With the improvement of response rate and tolerability of this treatment chronic hepatitis C with normal liver function has become widely accepted as the treatment indication. The recently introduced DAAs have raised response rates, and triple therapy with a DAA added to peginterferon and ribavirin combination therapy is already accepted as the optimal therapy for genotype 1 in AASLD guideline.3 It could soon become the standard therapy.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print




